DEPARTMENT
OF
THE
NAVY
/
\\
COMMANDER
NAVY
RESERVE
FORCE
fl
i9i5
FORRESTAL
DRIVE
—
NORFOLK
ViRGINIA
23531—4615
6000
COMNAVRESFOR
N9
23
Mar2020
Changes
to
the
identified
Navy
Reserve
Personnel
Manual
articles
are
effective
the
date
written
at
the
top
of
each
article
and
the
date
on
this
change
summary.
J.
A
SCHOMMER
Deputy
Commander
Changes
in
articles
titled
and
summarized
below
are
incorporated
in
the
electronic
copy
via
Commander,
Navy
Reserve
Forces
Command
(COMNAVRESFORCOM)
Website:
https://www.navyreserve
navy.mil.
Table
of
Contents
—
Revised
to
reflect
all
current
changes
Article
No.
Article
Title
6000-010
Reserve
Medical
.
Clarifications
of
Total
Force
IMR
percentage
theresholds.
.
New
requirements
for
Hepatitis
C
virus
titer
requirements
for
service
members
born
between
the
years
1945-1
965.
.
Clarification
of
Deployment
Health
Assessment
(DHA)
tracking
requirements.
•
Clarification
of
Injury
Case
Management
requirements.
•
New
requirements
for
DHA
reporting
for
sexual
assault
cases.
•
Additional
guidance
on
Pregnancy
Administration
management.
.
Updated
requirements
IRT
Mattis
memo
on
DoD
Transgender
Policy.
CHANGE
SUMMARY
March
2020
Page
lofI
RESPERSMAN
6000-0
10
6000-0
10
(Mar
2020)
Page
1
of
11
RESERVE
MEDICAL
Responsible
COMNAVRESFOR
(N9) Phone:
DSN
262-5643
Office
COMM
(757)
322-5643
FAX
(757)
444-7545
References
(a)
DoDI
6025.19
(IMR)
:
(b)
MILPERSMAN
1910-158
(Separation
for
the
Ready Reserve)
(c)
NAVADMIN
233/07
(IMR)
(d)
SECNAVINST
7850.4E (Disability
Evaluation
Manual)
(e)
SECNAVINST
5300.30F
(HIV,
HBV,
HCV)
(0
NAVADMIN
070/19
(Transgender)
(g)
OPNAVINST
6100.3A
(DHA
Process)
(h)
BUMEDThJST
1300.3
(Suitability
Screening)
(i)
RESPERSMAN
1300-0
10
(j)
MANMED
CH
15, 16,
18
and
23
(k)
BUPERSINST
l001.39F
(ADMIN
Procedures)
(I)
SECNAVINST
1770.5
(LOD)
(m)
COMNAVRESFORINST
6000.IE
(Pregnancy)
Enclosures
(1)
Manpower
Availability
Status Codes
(2)
HS-1
Force
Health
Protection
and
Readiness Checklist
1.
Background.
Commander.
Navy
Reserve
Force
(COMNAVRESFOR)
Force Surgeon
will
establish
policy
and
issue
guidance
for
Navy
Reserve
Force
Health
Protection
and
management.
Subordinate
echelons
Navy
Reserve
Activity
(NRA)
Commanding
Officers
(COs),
Officers
in
Charge
(OICs)
and
Unit
Leaders
will
ensure
Reserve
Force
Health
protection policy
and
guidance
parameters
are
met.
2.
Responsibilities
a.
NRAs
must:
(1)
Ensure
drilling
Reservists
and
Strategic
Sealift
Readiness
Group
members
complete
all
Individual
Medical Readiness
(IMR)
requirements
per
reference
(a).
Failure
to
report
for
required
IMR
needs
after
the
members
required
annual
update
may
result
in
the
member
being
processed
for
separation
by
reason
of
unsatisfactory
participation
per
reference
(b).
(2)
Educate
members
on
their
responsibility
to
submit
any
changes
regarding
their
health
or
medical
condition
within
60
days
of
diagnosis.
6000-0
10
(Mar
2020)
Page
2
of
11
(3)
Refer
members
who
fail
to
disclose medical
conditions
for
administrative
separation,
in
accordance
with
reference
(b).
b.
Unit COs/OIC
must:
(I)
Ensure
their
personnel
are
in
compliance
with
IMR
requirements
in
accordance
with
reference
(a).
(2)
Ensure
the
medical
readiness
of
individual
service members
is
considered
during each
clinical encounter,
and
monitored
for
compliance
as
per
reference
(c).
(3)
Inform
the
supporting
NRA
Medical
Department Representative
(MDR)
of
members’
deployment
limiting
medical
and
dental
condition,
and
or
changes
in
existing conditions,
that
might
interfere
with
their ability
to
perform their
duties.
(4)
Ensure
members
are
in
compliance
with
all
injury
case
management
requirements.
c.
NRA
MDR
must:
(I)
Have
a
current
assumption
of
duty
letter,
and
an
all-inclusive
medical
department
turnover assessment
and
evaluation
of
its
status
within
30
days
of
assumption
of
duty.
(2)
Maintain
a
Standard
Operating
Procedures
(SOP)
as
outlined
in
COMNAVRESFORINST
5040.1.
The
SOPs
should
incorporate
local
Department
of
Defense
(DoD)
MTFs’
guidance,
processes,
and
protocols
as
applicable.
(3) Notil’y’the
Unit
CO/OIC
of
the
NRA CO’s
determination
of
injury
management
and
drill
or
non-drill
status.
(4)
Ensure
every
injury
case
has
a
separate
file
from the
service treatment
records
(STR).
Update Medical Readiness
Reporting
System
(MRRS)
status
tab
in
detail
regarding
the case.
(5)
Communicate regularly
(minimum
monthly)
with
members
with
open
injury
cases.
(6)
Educate
members
on
their responsibility
to
submit
any
changes
regarding
their
medical
and
or
dental
condition
within
60
days
of
diagnosis.
(7)
Refer
members
who
fail
to
disclose
any
health
conditions
for
administrative separation,
in
accordance
with
reference
(b).
(8)
Submit
dental
treatment information
on
NAVMED
6600/12.
(9)
Educate
members
on
PERS-95
determinations
and
election
of
options per
PERS
official
message.
Per
RESPERSMAN
1300-050,
members
requesting
a
Physical
Evaluation
Board
(PEB)
must
be
transferred
to
the
Administrative
Processing
Unit
and
are
not
authorized
to
drill
until
the final
disposition
of
their
ease
is
made by
the PEB.

6000-0
10
(Mar
2020)
Page
3
of
11
(10)
Request
extensions
of
Temporary
Not
Physically/Dentally
Not
Qualified
(ThPQ/TNDQ)
cases
less
than
180
days
from
echelon
four (N9),
via
MRRS.
Members
who
fail
to
comply
with
medical
or
dental
requirements
may
be
processed
for
separation
by
reason
of
unsatisfactory
participation
per
references
(b)
and
(d).
(11)
Notify
NRA
Manpower
Department
of
the
appropriate
Manpower
Availability
Status
(MAS)
code
for
any
changes
in
member’s
medical
or
dental
status.
(12)
In
case
of
non-compliance,
appropriately
notify members
and
Chain
of
Command
(CoC)
(pg.
13,
certified
mail,
internal
tracking).
(13)
Refer
members
who
fail
to
comply
when
notified
to
the
administration
department
for
separation
process.
Maintain
non-compliance
files
for
a
minimum
of
two
years.
(14)
Be
notified
of
personnel
gains
and
losses from
the
manpower
department.
Monthly
reconciliation
reports
should
be
conducted
utilizing
command Alpha
Roster
and
MAS
Code
Accountability
reports
with
the
Navy
Standard Integrated
Personnel
System
(NSIPS)
operator.
(15)
Utilize
MRRS
to
track
IMR.
Track
completion
of
IMR
requirements
to
reflect
current
standards.
a.
Fully
Medically
Ready
85%.
b.
Partially
Medically Ready
S5%.
c.
Medically Ready
Indeterminate
5
5%.
d.
Not
Medically
Ready
S
5%.
e.
Full
+
Partial
Medical
Readiness
?
90%.
(16)
Ensure
Reserve
personnel
are
screened
every
24
months
for
serologic
evidence
of
Human
Immunodeficiency
Virus
(HIV),
one
time
for
Hepatitis
C
Virus
(HCV) for
members
born
between
the
years
1945
and
1965,
and
otherwise
for
HIV,
Hepatitis
B
Virus
(HBV),
and
HCV
as
clinically
indicated.
Additionally,
Reserve
members
will
be
tested
for
HIV
and
HCV
(for
members
born
between
the
years
1945
and
1965)
at
the
time
of
activation when
called
to
active
duty
for
more
than
30
days
if
they
have
not
been
tested
within
the last
24
months,
per
reference
(e).
(17)
Have
direct
access
to
the
NRA
CO
and
communicate
with
leadership
about
any
medical
and
dental
requirements,
deficiencies,
and
status
of
injury
cases.
(18)
Verify
all
medical
and
dental
records
STRs
in
accordance
with
MANMED
Chapter
16,
and
ensure
proper
disposition
of
all
STRs
within
five
days
of
separation
date
or
VA
request.
(19)
Screen
mobilizing
members
for
suitability
per
current
Area
of
Responsibility
(AOR)
guidance. Submit
AOR medical waivers
to
appropriate
AOR surgeon
via the
Reserve
Component
Command
(RCC).
6000-0
10
(Mar
2020)
Page
4
of
11
(20)
Recommend
to
NRA
CO
whether
a
member
should
be
placed
in
a
TNPQ,
TNDQ,
Line
of
Duty (LOD),
or
Medical
Retention
Review
(MRR)
status,
and
advise
on
drill
or
non-drill
status.
(21)
Ensure
members
are
completing
the
required Pre-DHA
DD
2795,
Post-DHA
DD
2796,
and
PDHRA
DD
2900
when
due.
Complete
deployment
screenings
via
EDHA,
document
in
MRRS,
and
place
in
members’
STRs.
(22)
Place
members
found
not
fit
on
the
Pre-DHA
in
the
appropriate
injury
case
management
status.
Manage
Post-DNA
and
Post-DHRA
referrals through
LOD
process.
(23)
Service
of
Transgender
Navy
Personnel,
per
reference
(O
who
received
a
diagnosis
of
gender
dysphoria
prior
to
12
April
2019,
who
wish
to
transition,
must
be
placed
TNPQ
with
MAS
code MPQ
given.
The
civilian
providers’
treatment
plan
must
be
reviewed
by
the
MDR
and
then
submitted
to
the Force
Surgeon,
who
will
then
fonvard
the
plan
for
validation
to
the
Navy
Transgender
Care
Team
(TGCT).
Once
the
treatment
plan
is
validated
by
the
TGCT.
the
member
submits
the
treatment
plan
as
part
of
the
overall
transition
plan
to
the
NRA
CO.
NRA MDR
will
consult
with
the
echelon
four
(N9)
regional
healthcare
providers
as
applicable.
d.
Navy
Reserve members
will:
(1)
Monitor
IMR
via
Bureau
of
Naval
Personnel
Online
and
comply
with
all
IMR
requirements
per
reference
(a)
and
(c).
(2)
Disclose
to
the
NRA
MDR
any
new
diagnosis, changes
in
existing
medical
conditions
and’or
prescription
medications’
dosage,
within
60
days
of
discovery.
3.
MDR
Trainine
Requirements
a.
Reserve
Medical
Administration
(RMA)
course
will be
completed
by
the
MDR
within
six
months
of
reporting
to
the
NRA,
and
every
five
years
thereafter.
RMA
curriculum
is
under revision
and
changes
will
affect
future
guidance.
b.
MDR
will
complete
the
Health
Insurance
Portability
and
Accountability
Act and
Privacy
Act
training within
30
days
of
checking
onboard,
and
annually
thereafter.
c.
MDR
will
complete
the
required
applicable
training
and
have
access
to
MRRS,
AHLTA/JLV/HAIMS,
MKS-Genesis,
EDHA,
VIALS,
PHA
portal,
ANACOMP,
and
NSIPS
STR,
WEB
WA
VE
II
(RCC
N9).
d.
TRICARE
training
course
is
required
every
two
years.
6000-0
10
(Mar
2020)
Page
5
of
11
e.
MDR
personnel
will
be
BLS
qualified.
Personnel
administering
vaccines
must
complete
at
least eight
hours
of
annual
continuing
education,
as
per
DHA-IHB reference
(g)
and
COMNAVRESFORCOM
guidance. Baseline
of
trainings
and
comprehensive immunization
standards
are
required
to
establish
competency.
Trainings
must
be
completed
upon
reporting
onboard,
and
every
three
years
thereafter. Training completion
must
be
verified
during
assessments
and
more
often
as
applicable
by
COMNAVRESFORCOM
and
echelon
four
(N9).
1’.
Resident
courses. Medical
personnel
may attend
the
Immunization
Lifelong
Learners
Course
(ILLC),
or
the
Immunization
Lifelong
Learners
Short
Course
(ILLSC).
These
resident
courses
will
satisfy
the
three-year
requirement.
g.
All
personnel
administering
seasonal
influenza
vaccination
will
complete
the
DoD
seasonal
influenza training
yearly.
Additionally,
personnel
will
provide
course
completion
yearly
for
each
additional
immunization
approved
for
and
supplied
to
the
NRA
outside
of
the
standard
readiness
immunizations
(example: Yellow
Fever).
h.
Blood-borne
Pathogen Training
course
via
ESAMS
as
required.
i.
During
inspections,
echelon
four
(N9)
will
utilize
the
most
current
COMNAVRES
FOR
5040.1
HS-1
Force Health
Protection
and
Readiness
Checklist
enclosure
(2) for
all
assessments
conducted
at
echelon
5
commands.
This
will
ensure
uniform
compliance
throughout
the
Reserve
Force.
4.
Deployment
Health
Assessment
a.
Assess
the
state
of
members’
health
after
deployment
outside
the
United
States
in
support
of
military operations
and
identify present
and
future
medical
care.
b.
Complete
the
required
Pre-Deployment
Health
Assessment
(Pre-DHA
DD
2795),
Post-
Deployment
Health
Assessment
(Post-DHA
DD
2796),
and
Post-Deployment
Health
Re
Assessment
(PDHRA
DD
2900)
per
reference
(g)
when
due.
c.
Review
all
members
with
a
deployment
history
for
completion
and
applicable
referrals.
d.
Psychological
Health
Outreach
Program (PHOP)
should
immediately
be
made
aware
of
any
referral
and
follow-up
needed.
e.
Ensure
deployment
health assessment
screenings
are
completed
via
EDHA,
documented
in
MRRS,
and
placed
in
members’
STRs.
f.
Identify
members
found
not
fit
on
the
Pre-DHA
DD
2795,
place
them
in
the
appropiate
injury
case
status,
and
assign
the
appropriate
MAS code.
g.
Manage Post-DHA
and
Post-DHRA
referrals through
the
LOD
process.
6000-0
10
(Mar
2020)
Page
6
of
11
5.
Injury
Case
Management
a.
Injury
cases
will
be
effectively
managed
and
updated
in
MRRS
to
reflect current
status,
updates,
and
details.
b.
For
members
in
an
injury
case status,
all
current,
signed
and
applicable documentation
must
be
available.
c.
Injury
case
file
will
be
available
for
each
case
and
will be
separate
from
STR.
d.
The
appropriate
MAS
Code
must be
assigned
at
opening
and
closing
of
all
injury
cases.
e.
Refer/recommend
for
TNPQ
and
TNDQ
as
appropriate.
(1)
Utilize
TNPQ
or
TNDQ
status
when
members
have
medical
or
dental
conditions
that
are
not
service
connected,
and
are
expected
to
be
resolved
in
less
than
180
days
per
reference
(i).
Members
in
this
status
must
be assigned
a
MAS
Code
of
MS3.
(2)
Members
in
TNPQ[FNDQ
status
must
provide
the
NRA
MDR
written
monthly
updates
on
their
treatment
progress
from
a
civilian
provider.
In
the
event
a
given
medical
or
dental
condition
does
not
require
a
clinical
visit
in
a
given
month,
TNPQ/TNDQ
members
must
still
contact
the
NRA
MDR.
Failure
to
comply
with
providing
monthly
updates
may
result
in
administrative
action,
non-compliance
letters,
and
administrative
separation
per
reference
(h).
(3)
The NRA
MDR
will
update
the member’s
medical record
and
MRRS
on
every status
change.
(4)
All
requests
for
extensions
of
TNPQ/TNDQ
will be
submitted
to
the
CoC
to
the
echelon
four
(N9)
for
approval
using
the
TNPQ
or
TNDQ
module
of
MRRS.
Extensions
of
TNPQ/TNDQ
should only be
for
cases
with
clear
expectation
of
complete
resolution,
otherwise
an
MRR
package
should
be
initiated
at
six
months.
No
extension
will
be
granted
beyond
365
days
without
the
approval
of
COMNAVRESFOR
Force
Surgeon.
(5)
Members
completing
their
plan
of
care
must
immediately
notify
the
NRA MDR
and
provide
all
current
documentation
in
support
of
their
course
of
treatment.
The
NRA
MDR
will
place
the
records
in
members’
STR
and
annotate treatment
completion
on
an SF
600.
Ordinarily,
completion
of
a
course
of
treatment
implies
resolution
and
the
TNPQ/ThDQ
status
can
be
removed
or
closed.
If
the
member’s
condition
still
exists after
365
days
the
condition
is
considered
chronic
and
the
TNPQ
must be
converted
into
a
MRR.
NRA
MDR
will
consult
with the
echelon
four
(N9)
regional
healthcare
providers,
and
elevate
queries
to
COMNAVRESFOR
Force
Health
department
(N9)
when
applicable.
6000-0
10
(Mar
2020)
Page
7
of
11
(6)
Inactive
Duty Participation
(a)
Members
in
a
TNPQ/TNDQ
status
are
eligible
to
perform
Inactive
Duty
Training
(IDT)
periods.
Coordination
between
TRUIC
NRA
and
Unit
Mobilization
Unit
Identification
Code
(UMUIC)
is
required
for
member
to
conduct
Inactive
Duty
Training
Travel
(IDTT) with
supported
command.
Members
may
request
consideration
for
IDTT,
Annual
Training
(AT),
and
Active
Duty
Training
(ADT).
TRUIC
NRA
CO,
in
conjunction
with
UMUIC
Unit
Leadership,
will
consider
these
requests
on
a
case-by-case
basis
and
may
approve
when
less
than
29
days
and
CONUS
assignment
based.
(b)
Members
in
TNPQ/TNDQ
status
are
assignable
in
accordance
with
reference
(i).
However,
members
will
remain assigned
to
their
administrative
NRA
and
in
Selected
Reserve
status
except
where
precluded
by
higher
policy
(e.g.
High
Year
Tenure,
Unsatisfactory
participation,
etc.)
(c)
Members
who
relocate
home
of
record
(HOR)
may
be
assigned
to
nearest NRA
in
accordance
with
reference
(i).
The losing NRA
must
contact
the
gaining
NRA
to
inform them
of
TNPQ/TNDQ
status
and
immediately
provide
all
medical
documentation
and
details.
(d)
Orthodontic
appliance
(braces)
and
or
orthognathic
treatment
(surgical
jaw
repositioning).
See
paragraph
(7)
below.
(7)
Members
who
decide
to
undergo active
orthodontic
treatment
and or
combined
orthodontic/orthognathic
treatment,
are
required
to
notify
their
Unit
CO/OIC
and
the
supporting
NRA
MDR.
The
NRA
MDR
will
educate
the
member
on
the
Navy’s
recall
and
deployment
policy
on
personnel
who
choose
to
undergo this
treatment,
and
sign
a
page
13
affirming
understanding.
Refer
to
NAVMED
1300/4,
Expeditionary
Medical
Screening Checklist
and
specific
AOR
requirements
for
restrictions
on
orthodontic
appliances
(8)
Members
undergoing
active
treatment
will
not
be
placed
TNDQ
or
classified
as
dental
class
three.
Members
can
be
dental
class
one
or
class two
and
be
under
active treatment.
Specific
deployment
requirements
will
dictate
if
members
who
execute
active duty
orders
greater
than
29
days
are
required
to
have
their
active
orthodontic
treatment
(braces)
deactivated.
The
member’s
treating
dentist
or
orthodontist
must
certify
that
the
member’s orthodontic
appliances
have
been
placed
in
a
stabilized
and
deactivated
status.
Members
choosing
to
undergo
combined
orthodontic/orthognathic
treatment must
be
placed
TNDQ
non-drill
status until
an
oral
surgeon
has
certified
all
surgical devices have
been removed
and
adequate healing
of
the
bones
and
jaw
have
occurred.
f.
Medical Retention Review
(MRR)
(I)
An
MRR
package
must
be
initiated
when the
NRA MDR
determines
that
a
member
has
developed
a
new
or
had
a
change
in an
existing
medical
condition,
that
is
chronic
in
nature,
and
will
likely
prevent
the
member
from
safely
and
effectively
thlfilling
duty
responsibilities,
and
or
interfere with
mobilization.
NRA MDR
will
consult
with
the
echelon four
(N9)
regional
healthcare
providers
to
determine
the
need
of
a
MRR,
and
elevate queries
to
COMNAVRESFOR
Force
Health
department
(N9)
if
applicable.
6000-0
10
(Mar
2020)
Page
8
of
11
(2)
The
NRA
MDR
has
60 days
to
gather
documentation
from
members,
for
package
completion
and
submission. Members
in an
MRR
status
are
required
to
submit
medical
documentation
within
30
days
of
a
medical
appointment.
Failure
to
comply
may result
in
administrative
action,
non-compliance
letters,
and
administrative
separation per
reference
(b).
(3)
The complete
MRR
package
will be
submitted
to
the
echelon
four
(N9)
for review,
quality assurance
(QA),
and
endorsement.
Echelon
4
commands
will
ensure
timely
upload
of
documents
into
the
electronic
databases
within
10
business
days,
and
monitor
package timelines
at
both
commands.
(4)
PERS-95
will
notify
the
member
of
their
findings
via
message
traffic.
Supporting
NRA
admin
department
must
notify
members
by
letter
via certified
mail
or
in
person
of
their
option
to
request
in
writing,
appeal
review by
the PER,
discharge,
or
transfer
to
the
retired
reserve
(if
eligible)
within
30
days
of
receipt
of
their
letter,
if
not
recommended
for
retention. MDR
will
ensure
members
are
notified
and
consult
with
their
NRA
admin
department
for
timely
processing.
(5)
Not
all
medical
conditions
require
a
MRR.
For
example,
if
the
condition
resolved
or
has
stabilized during
TNPQ
status, has
not
had any
change
in
the
past
90
days,
and
does
not
need
a
waiver
submitted
to
the
AOR per
CENTCOM
MOD
series
and
AFRICOM requirements,
then
a
MRR
package
does
not
need
to
be submitted.
These
conditions
still
requires that
appropriate
documentation
from
the
treating provider
as
well
as
a
SF
600
entry
outlining
decision
considerations
be placed
in
the medical
record.
Members
must report,
within
60
days, any
new
condition
or
changes
in
existing conditions, including
prescription
medications’
dosage
changes.
(6)
BUMED
will
review the MRR
package
and
determine
the
physical
qualification
status
per
reference
(h):
(a)
Physically
Qualified
(PQ):
Unrestricted
IDT,
IDTT,
AT,
and
ADT.
No
MAS
Code.
(b)
Not
Physically
Qualified/Retention
Recommended
(NPQ/RR): OCONUS
and
greater
than
30
days
CONUS
assignment
requires
an
AOR
Waiver
from
gaining
command surgeon.
Less
than
30
days
CONUS approval
is
at
the
CO’s
and
unit
OIC’s
discretion,
with
MDR
input/discretion.
CoC
will be
utilized
for
any
questions.
PERS
message
will
specify
administrative
requirements,
restrictions,
and
ffiture
submission
requirements.
(c)
Not
Physically Qualified/Retention
Not
Recommended
(NPQ/RNR): Member
may
complete
correspondence
courses
only.
May
be
assigned
an
administrative
MAS
code.
(ex.
AAP
or
AAR).
(7)
Inactive Duty
Participation
(a)
Members
in
an
MRR status,
awaiting
BUMED
review,
are
only
eligible
to
perform
IDT
periods
at
TRUIC
NRA
CO
and
Unit
leadership
discretion per
reference
(k).
Refer
to
paragraph
b.
regarding
further
participation
guidance
once
the
MRR package
has
been
adjudicated
and
member
is
in
a
NPQ/RR
status.
6000-0
10
(Mar
2020)
Page
9
of
11
(b)
Members
in
MRR
status, awaiting
BUMED
review,
are
unassignable
in
accordance
with
RESPERSMAN
1300-010.
However, members
shall
remain assigned
to
their
unit,
except
where precluded
by
higher
policy
(e.g.
High
Year
Tenure,
Unsatisfactory participation,
etc.)
(c)
Members
who
relocate
HOR
may
be
assigned
to
nearest NRA
in
accordance
with
reference
(j).
The
losing
NRA
shall
contact
the
gaining
NRA
to
inform them
of
MRR
status
and
immediately
provide
all
medical
documentationlMRR
package
status.
g.
Line
of
Duty (LOD)
(I)
Utilize
LOD
cases
for
Reserve members
who
incur
or
aggravate
an
illness,
injury,
or
disease
that
qualifies
for
benefits under
the
SECNAVINST
1770.5.
(2)
LOD
benefits
are
available
to
eligible Reserve
members
and
may
include
inpatient
or
outpatient
healthcare,
dental
care,
Incapacitation
Pay
(INCAP
Pay),
travel
and
transportation
allowance,
separation
pay,
or
disability
retirement.
(3)
Each
case
will
be
opened
and
submitted
within
180
day
of
injury
or
condition’s
discovery.
LOD
requests,
monthly
updates,
appeals
and
INCAP
Pay
requests
must
be
submitted
to
the
respective echelon
4
(N9) for
review
and
accuracy,
utilizing
the
LOD
Checklist.
Once
complete,
requests
will
be
submitted
to
PERS-95.
(4)
Ensure
the
members
understand
that
the
requirements
of
an
LOD and
that
the
MEB/PEB
processes
are
initiated
as
directed by
the
Benefits Issuing
Authority
(BIA).
(5)
MDRs should make
recommendations
(DD
Form
261)
on
whether
or
not
members
can
perform
military
duties
(drilling
or
non-drilling).
(6)
Appeals
will
be
forwarded
to
Office
of
the
Judge Advocate
General
(OJAG)
with
PERS
95’s
recommendation.
(7)
INCAP
Pay
is
reviewed
and
forwarded
to
DFAS.
PERS-95
does
not
determine
the
amount
of
money
members
will
receive.
(8)
Members with
open
LODs
must
provide
written
monthly
updates
on
their
treatment
progress
to
their NRA
MDR
from
their
medical provider.
If
a
medical
or
dental
condition
does
not
require
a
monthly
clinical
visit,
LOD
members must
still
contact
the
NRA
MDR
each
month.
(9)
Failure
to
comply
may result
in
administrative
actions,
non-compliance
letters,
and
administrative separation
per
reference
(b).
Reference
(k)
serves
the
guide
for
proper package
compilation
and
submission
processes. Members
in
a
flight
status
that
are
placed
LOD
must
be
issued
a
grounding
notice,
DD
2992,
JAN
2015.
6000-0
10
(Mar
2020)
Page
10
of
11
(10)
Inactive Duty
Participation
(a)
Members
who
have
an
approved
LOD
may
request
consideration
for
1D17,
AT,
and
ADT
via
PERS-95.
PERS-95
must
consider
these
requests
on
a
case-by-case
basis
and
may
approve
when
less
than
29
days
and
CONUS
assignment
based. Members
in
an
LOD
status
are
eligible
to
perform
IDT
periods
at
TRUIC
NRA
CO
and
Unit
Leadership
discretion.
(b)
Members
in
a
LCD
status
are
unassignable
in
accordance
with
reference
(I).
However,
members
must
remain
assigned
to
their
unit,
except
where
precluded
by
higher
policy
(e.g.
High
Year
Tenure,
Unsatisfactory
participation,
etc.)
(c)
Members
who
relocate
HOR
may
be
assigned
to
nearest
NRA
in
accordance
with
reference
(j).
The
losing
NRA
must
contact
the
gaining
NRA
to
inform
them
of
LCD
status
and
immediately
provide
all
medical
documentation
and
process
status.
h.
MedHold
(I)
MedHold
is
a
voluntary
medical
treatment
program
for
Reserve
members
with
the
sole
purpose
of
addressing
medical
conditions
incurred
or
aggravated
while
in
the
LCD.
Evidence
must
exist
in
the
member’s medical
records
that
the
condition
was
identified
and
documented
while
the
member
was
in
a
duty
status.
Once
eligibility
has
been
determined,
members
may
request
or
accept
MedHold
orders.
(2)
The
mere
existence
of
an
illness,
injury
or
disease
does
not
necessarily
qualify
a
service
member
for
MedHold.
The
condition
must
be
deemed
potentially
unfitting,
as
determined
by
their
respective
service.
(3)
MedHold
request packages
will
be
submitted
via
their
COl
to
be
forwarded
to
PERS-95
for
review.
This
is
not
a
requirement
of
PERS-95.
(4)
The MDR
is
responsible
for
proper
submission
of
the
request.
Incomplete
MedHold
request
packages
will
not
be
processed,
and
requests
will
be
delayed
until
receipt
of
missing
documents.
(5)
Sailors
on
MedHold
greater
than
12
months
and
not
found “Fit
for
duty”
will
be
directed
to
a
MEB/PEB.
i.
Sexual
Assault
Prevention
and
Response
(SAPR)
(1)
Sexual
Assault
Unrestricted
cases
will
be
sent
to
lod
sapri3,navy.mil
to
ensure
preservation
of
privacy.
(2)
Investigation
documents
are
needed
if
the
member
requesting
benefits
is
being
investigated
for
misconduct.
(3)
Sexual
Assault
Restricted
cases
will
be
submitted
directly
to
Defense
Health
Agency
(DHA).
Do
not
open
a
LCD
in
MRRS
as
these
cases
are
tracked
by
DHA.

60
00-0
10
(Mar
2020)
Page
11
of
11
j.
Pregnancy
Administration
Management
(1)
Manage
and
update
MRRS
to
reflect
current
status.
(2)
Inform
COC
and
elect Drill,
Non!Drill
options.
(3)
Service
member
must
confirm
pregnancy
through
a
medical
provider
at
either
a
MTF
or
a
civilian facility.
Ensure
members
have
medical
documentation
indicating
prospective
due
dates
and
any
restriction.
(4)
Educate
pregnant
members
and
ensure
they
are
familiar
with
their
responsibilities.
(5)
Monitor
due
dates
in
MRRS
and
any
change
in
delivery
date
per
reference
Q.
(6)
Maintain
files
for
a
minimum
of
two
years.
Reports
should account
for
all
pregnant
personnel
and
correct
assignment
of
MAS
codes.
(7)
Verify
and
take
necessary
action
if/when
pregnant
members
perform
active
or
inactive
duty
training
per
reference
(m).
(8)
Obtain
return
to
duty/clearing
documentation
from
member.
Update
status
in
MRRS
and
monitor
MAS
code.

Supplemental MAS Code Guidance for
RESPERSMAN M-1001.5
Updated 01 NOV 2019
Enclosure (1)
MANPOWER AVAILABILITY STATUS (MAS) CODES
This document provides additional guidance to supplement MAS
code instructions found in RESPERS M-1001.5, Navy Reserve
Personnel Manual (RESPERSMAN). MAS codes are used by the Navy
Reserve Force to identify a Sailor’s readiness to mobilize.
Therefore, MAS code accuracy is the essential tool Commanding
Officers use to communicate the readiness of their Sailors to
COMNAVRESFORCOM. Echelon IV and V manpower and mobilization
officers shall familiarize themselves with and ensure adherence
to this guidance. Any questions concerning MAS codes should be
directed to COMNAVRESFORCOM N35.
NSIPS allows the tracking of three categories of MAS codes:
Medical, Administrative, and Training. Current NSIPS
programming does not recognize MAS code relative precedence
order; therefore, when assigning MAS codes, Echelon IV and V
commands shall follow the order of precedence provided in each
category: Medical, Administrative, and Training.
Most MAS codes are assigned a periodicity. COMNAVRESFORCOM N35
will post on its website those MAS codes that are past the
periodicity and those MAS codes that are approaching the
periodicity.
There are four MAS codes reserved for COMNAVRESFORCOM use only.
AKE, SAD, and PRO are controlled by COMNAVRESFORCOM N35. DCO is
controlled by COMNAVRESFORCOM N7. If there are any discrepancies
with these codes, contact COMNAVRESFORCOM N35/N7 respectively.
When a Sailor has an IMS code under the “mobilization
processing” or “activation status” IMS code categories, the
Sailor’s record is locked. A locked record prevents MAS code
changes and separations. If an update to a record that is
locked needs to be made, contact COMNAVRESFORCOM N35 for
assistance.
1. Medical/Dental MAS Codes: The following Medical/Dental MAS
codes are used to report and track potential medical/dental
issues that may preclude a Reserve Sailor from executing active
duty orders. These codes are listed in precedence order from
highest to lowest precedence.
Note: RC Sailors assigned medical/dental MAS codes are expected
to aggressively correct the issue resulting in assignment of the
MAS code. Members that Fail to Disclose a mobilization-limiting
medical or dental condition will be transferred to S-2 status in

Supplemental MAS Code Guidance for
RESPERSMAN M-1001.5
Updated 01 NOV 2019
Enclosure 1
accordance with COMNAVRESFORINST 3060.7 series.
MAS
Prec Code Definition
1 MPQ Not qualified for retention; currently undergoing PEB.
An MRR submitted that receives Not Physically
Qualified/Retention Not Recommended (NPQ/RNR) after
BUMED review and has requested a PEB will receive the
MAS code MPQ once that package is submitted to the
PEB. May result in AAP or ARR Administrative MAS
code. References NAVMED P-117, RESPERSMAN 6000-010,
and MILPERSMAN 6110-020. (180 days)
2 MS2 Medical Retention Review (MRR) initiated. References
NAVMED P-117, RESPERSMAN 6000-010, and MILPERSMAN
6110-020. (180 days)
3 MS1 Line of Duty (LOD) Initiated. References SECNAVINST
1770.3 (series), NAVMED P-117, RESPERSMAN 6000-010,
and MILPERSMAN 6110-020. (365 days).
4 MS3 Temporarily Not Physically Qualified (TNPQ). MRR or
Physical Evaluation Board (PEB) is not required or has
NOT yet been submitted. Reference MILPERSMAN 6110-020
and RESPERSMAN 6000-010. (180 days)
5 MPC Pregnant. Reference OPNAVINST 6000.1C. (294 days)
6 MPP Non-deployable mother, child less than 12 months old
or postpartum convalescence. This MAS code does not
preclude a Sailor from being tagged for an involuntary
mobilization as long as the Ready Load Date (RLD) is
after the deferment expiration date. A Sailor may
waive this requirement. Reference OPNAVINST 6000.1C.
(365 days - automatic removal)
7* MNN An MRR submitted that receives Not Physically
Qualified/Retention Recommended (NPQ/RR) after Bureau
of Medicine and Surgery (BUMED) review will receive a
MAS code of MNN. Anyone with an MNN MAS code is not
qualified for orders greater than 30 days without an
approved Area of Responsibility (AOR) waiver.
Approval for anything INCONUS less than 30 days is at
the CO/OIC’s discretion, with MDR input. AOR waivers
are required for OCONUS orders of any length.
References MILPERSMAN 6110-020 and RESPERSMAN 6000-
Supplemental MAS Code Guidance for
RESPERSMAN M-1001.5
Updated 01 NOV 2019
Enclosure 1
010. (365 days)
8* MDT Dental Class III which does not preclude mobilization.
References SECNAVINST 6120.3 CH-1 and RESPERSMAN 6000-
010. (180 days)
9* MDF Dental Class IV which does not preclude mobilization.
References SECNAVINST 6120.3 CH-1 and RESPERSMAN 6000-
010. (180 days)
* MAS code does not preclude mobilization
2. Administrative MAS Codes: The following administrative MAS
codes are used to report and track administrative issues that
may preclude a Reserve Sailor from executing active duty orders.
MAS
Prec Code Definition
1 BCG BUPERS Control Group. Member’s record is frozen by
PERS-834 or PERS-911D. Contact PERS-83/911D to
inquire.
2 AKE Key Federal Employee (COMNAVRESFORCOM N35 use only).
References DoD Directive 1200.7 and BUPERSINST
1001.39F.
3 AUP Unsatisfactory participant. Reference RESPERSMAN
1001-010. (180 days)
4 ACR Member has an approved conditional release from the
Navy Reserve. Remove upon enlistment/appointment or
expiration. References BUPERSINST 1001.39F and
MILPERSMAN 1910-102. (180 days)
5 AAP Administrative action pending which would preclude
mobilization (e.g., un-adjudicated administrative
separation (ADSEP) other than for UNSAT participation,
Navy Reserve Activity (NRA) received Individual Ready
Reserve (IRR) request, pending transfer from Select
Reservist (SELRES) to Full-Time Support (FTS) or
Active Component, pending acceptance into a
commissioning program, etc.). Code applied upon
signature/submission to approval authority. Remove
immediately if request/application is denied or
withdrawn. Reference RESPERSMAN 1001.5. (180 days)
Supplemental MAS Code Guidance for
RESPERSMAN M-1001.5
Updated 01 NOV 2019
Enclosure 1
6 ASF Member is ineligible for force protection duties.
Member has a conviction in any court of a misdemeanor
or felony crime of domestic violence. References
Lautenberg Amendment, Section 922(g)(9) of Title 18,
U.S.C., DoDI 6400.06, and DD FORM 2760. Per
MILPERSMAN 1910-142, member must be processed for
separation (AAP MAS code applies). Apply ASF MAS code
if member has completed the separation process, but is
retained. Also apply the AFP if a member has
allergies related to pepper or a pre-existing history
of allergic reaction when exposed to pepper or
Oleoresin Capsicum (OC) pepper spray. Reference Navy
Security Force Sentry prerequisites (A-830-2216).
7 APB Enlisted probationary drill status (UNSAT). NRA has
six months to declare member in good drill standing or
ADSEP for UNSAT participation IAW BUPERSINST 1001.39F,
MILPERSMAN 1001-150, and RESPERSMAN 1001-010. (180
days)
8 ARR Retirement request submitted to NRA and pending
approval from PERS-9, or retirement request approved
by PERS-9. Reference MILPERSMAN 1810-020. (365 days)
9 ACB Member not selected for continuation. Enlisted
reference current Senior Enlisted Continuation Board
NAVADMIN. Officer reference SECNAVINST 1920.7C and
http://www.public.navy.mil/bupers-
npc/career/reservepersonnelmgmt/officers/Pages/Continu
ation.aspx. (365 days)
10 AS2 Member is within six months of High Year Tenure (HYT)
or statutory attrition. If the member transfers to
the VTU, transfers to the IRR, or retires, remove this
MAS code. Enlisted reference MILPERSMAN 1160-120 and
http://www.public.navy.mil/bupers-
npc/career/reservepersonnelmgmt/enlisted/Pages/HYT.aspx.
Officer reference SECNAVINST 1920.7C and
http://www.public.navy.mil/bupers-
npc/career/reservepersonnelmgmt/officers/Pages/Attriti
onRetirement.aspx. (180 days)
11 TS1 Member who affiliated within 183 days of release from
Active Duty (Navy or other Service) and is authorized
a 24-month deferment from involuntary mobilization,
commencing on the date of affiliation with the Navy
Reserve. This MAS code does not preclude a Sailor
Supplemental MAS Code Guidance for
RESPERSMAN M-1001.5
Updated 01 NOV 2019
Enclosure 1
from being tagged for an involuntary mobilization as
long as the Ready Load Date is after the deferment
expiration date. Sailors
may volunteer for
mobilization at any time during
this deferment by
signing a NAVPERS 1070/613, waiving their deferment
period. Deferment does not apply to long-term
operational support orders (e.g., ADSW, ADT, RECALL,
etc.) or New Accession Training (NAT) Sailors.
Reference NAVADMIN 145/19. (730 days - automatic
removal)
12 AS1 Member who affiliated with prior military service
(Navy or other Service, including members of the IRR
or VTU) and is authorized a one-time 12-month
deferment from involuntary mobilization
commencing on
the date of affiliation with the Navy Reserve. This
MAS code does not preclude a Sailor from being tagged
for an involuntary mobilization as long as the RLD is
after the deferment expiration date. Sailors may
volunteer for mobilization at any time during this
deferment by signing a NAVPERS 1070/613, waiving their
deferment period. Deferment does not apply to long-
term operational support orders (e.g., ADSW, ADT,
RECALL, etc.) or NAT Sailors. Reference NAVADMIN
145/19. (365 days - automatic removal)
13* ASO Sole surviving son or daughter. Reference DoDI
1315.18. This code limits locations for mobilization.
14* AFP Joint Personnel Adjudication System (JPAS) records
indicate derogatory eligibility determination, to
include: Administrative Withdrawal, Loss of
Jurisdiction, Revoked or Denied eligibility, No
Determination Made, or currently reporting an active
incident report. If eligibility determination has not
been finalized by Department of the Navy Central
Adjudication Facility (DoNCAF), the AFP code should
not be automatically assumed as the member may have
been granted INTERIM access by the owning command, in
which case the member could still be eligible for
continued access and mobilization. References DoD
Directive 5200.2 and SECNAVINST M-5510.30.
15* ASP Member is a single parent or guardian and requires a
family care plan. References OPNAVINST 1740.4D and
OPNAVINST 6000.1C.

Supplemental MAS Code Guidance for
RESPERSMAN M-1001.5
Updated 01 NOV 2019
Enclosure 1
16* ASD Member has an Active/Reserve military spouse and
requires a family care plan. References OPNAVINST
1740.4D and OPNAVINST 6000.1C.
17* AS3 Member is a non-custodial single parent who does not
require a family care plan. References OPNAVINST
1740.4D and OPNAVINST 6000.1C.
18* MPT Member failed most recent PFA. References OPNAVINST
6110.1 (series), NAVADMIN 304/17, and ALNAVRESFOR
012/18. (180 days)
19* OAT Member’s GTCC card is either currently revoked or
suspended. Code removed immediately upon
reactivation/reissue of GTCC. Reference DoDI 5154.31,
Volume 4. (365 days)
* MAS code does not preclude mobilization
3. Training MAS Codes: The following training MAS codes are
used to report and track Reserve Sailors that are in special
training programs or who have not completed all training
required by law, DoD directive,
or other directives and
instructions.
MAS
Prec Code Definition
1 SAD Approaching sanctuary. Member has 16 years or more of
Active Duty. Calculated by the total accumulation of
Active Service (AT + ADT + ADSW + Mobilization +
Recall + USN + FTS + Any other active duty time).
Reference OPNAVINST 1001.27. (COMNAVRESFORCOM use
only – do not remove without contacting
COMNAVRESFORCOM N35).
2 TMS Attending authorized medical or dental school which
results in the awarding of the degree of Medical
Doctor (M.D.), Doctor of Osteopathy (D.O.), Doctor of
Dental Surgery (D.D.S.), Doctor of Dental Medicine
(DMD), or equivalent as determined by the BUMED
Reserve Affairs Officer (RAO). TMS requires a letter
designating and verifying the Member has been accepted
into the program from BUMED IAW RESPERSMAN 1570-020.
Without BUMED RAO approval, Member will be mobilized
under his/her current designator or rating. (1460
days)
Supplemental MAS Code Guidance for
RESPERSMAN M-1001.5
Updated 01 NOV 2019
Enclosure 1
3 DCO For COMNAVRESFORCOM HQ use only. DCO MAS code will be
added by COMNAVRESFORCOM N7 upon commissioning and
removed by COMNAVRESFORCOM N7 upon completion of
Direct Commission Officer Indoctrination Course
(DCOIC) per RESPERSMAN 1200-010. Per COMNAVRESFORINST
1120.3 series LDOs/CWOs/DCOs are required to attend
DCOIC within one year of commissioning. (365 days)
4 TBH Member, either officer or enlisted, has not completed
prescribed community specific training or necessary
requirements for appropriate certification,
credentialing, privileging, or clinical support
assignment/clinical sustainment as a healthcare
professional to be considered qualified for
mobilization. For officers, upon completion of DCOIC
and removal of DCO MAS code, the TBH MAS code will be
assigned to those with follow-on accession training by
their NRA in accordance with the DCO accession
training guidance available on the COMNAVRESFORCOM N7
DCO homepage. Upon completion of accession training,
DCOs will provide proof to their Unit CO and NRA CO to
ensure the TBH MAS code is removed. Reference
COMNAVCRUITCOMINST 1130.8 and RESPERSMAN 1300-080.(730
days)
5 PRO SELRES Officer who was authorized early release from
Active Duty service obligation to participate in a
United States professional sport league. Reference
DoDI 1322.22. (365 days)
6 TS2 RP assigned to USMC unit, but has not received NEC
2401, Marine Basic Combat Skills Specialist (A-561-
0008). Reference MCO 1730-6D. (365 days)
7 TRP PRISE-R/designator or rate conversion training,
assigned IAW MILPERSMAN 1133-061. (545 days)
8* VS1 Member is on Definite (Temporary) Recall.
9* OWS Member is on ADOS/ADSW. NRA will assign code upon
member departing on orders and will remove the
code
when member returns to the NRA.
10* VOL Member is a volunteer and fully available/ready for
mobilization. Member volunteering for a mobilization
Supplemental MAS Code Guidance for
RESPERSMAN M-1001.5
Updated 01 NOV 2019
Enclosure 1
should volunteer through COMNAVRESFORCOM N35’s website
or contact N35 directly.
* MAS code does not preclude mobilization
4. Spare or no longer used MAS codes: The following list of MAS
codes are either spares or no longer in use. The Spares are for
COMNAVRESFORCOM N35 use only.
MAS Code
Spare/Previous Definition
MP1 Medical spare
OTN On ADT less than 180 days not in support of OPS
OTS On ADT less than 180 days in support of a crisis
TBX Training Spare 5
TCB Training Spare 1
TDX Completed IADT
THS For Headquarters use only. Mobilization Capacity
Hold
TRL Attend valid rel trng-1405 Desig, period 730 days
TS3 Officer assgn Chapliain Cand Prgm
TSP Stipend participation
VLI Volunteer for INCONUS only
VLO Volunteer for OCONUS only
VLU Volunteer to go with assigned Unit only
VS2 Volunteer spare
Enclosure 1
Per current policy, shaded MAS codes do not preclude mobilization.
# MAS Code has automatic removal upon expiration.
CODE
Description
Precedence
Periodicity
Controlling Authority
MEDICAL
MPQ
Not physically qualified for mobilization; PEB has been initiated.
1
180 days
NAVMED P-117, RESPERSMAN 6000-010, and
MILPERSMAN 6110-020
MS2
MRR initiated.
2
180 days
NAVMED P-117, RESPERSMAN 6000-010, and
MILPERSMAN 6110-020
MS1
Temporarily not physically qualified for retention. MRR or PEB package has been submitted. Final
adjudication of MRR or PEB package has not been received. MS1 shall be assigned when the MRR or
PEB package is submitted to allow tracking of package through adjudication.
3
365 days
SECNAVINST 1770.3 (series), NAVMED P-117,
RESPERSMAN 6000-010, and MILPERSMAN 6110-020
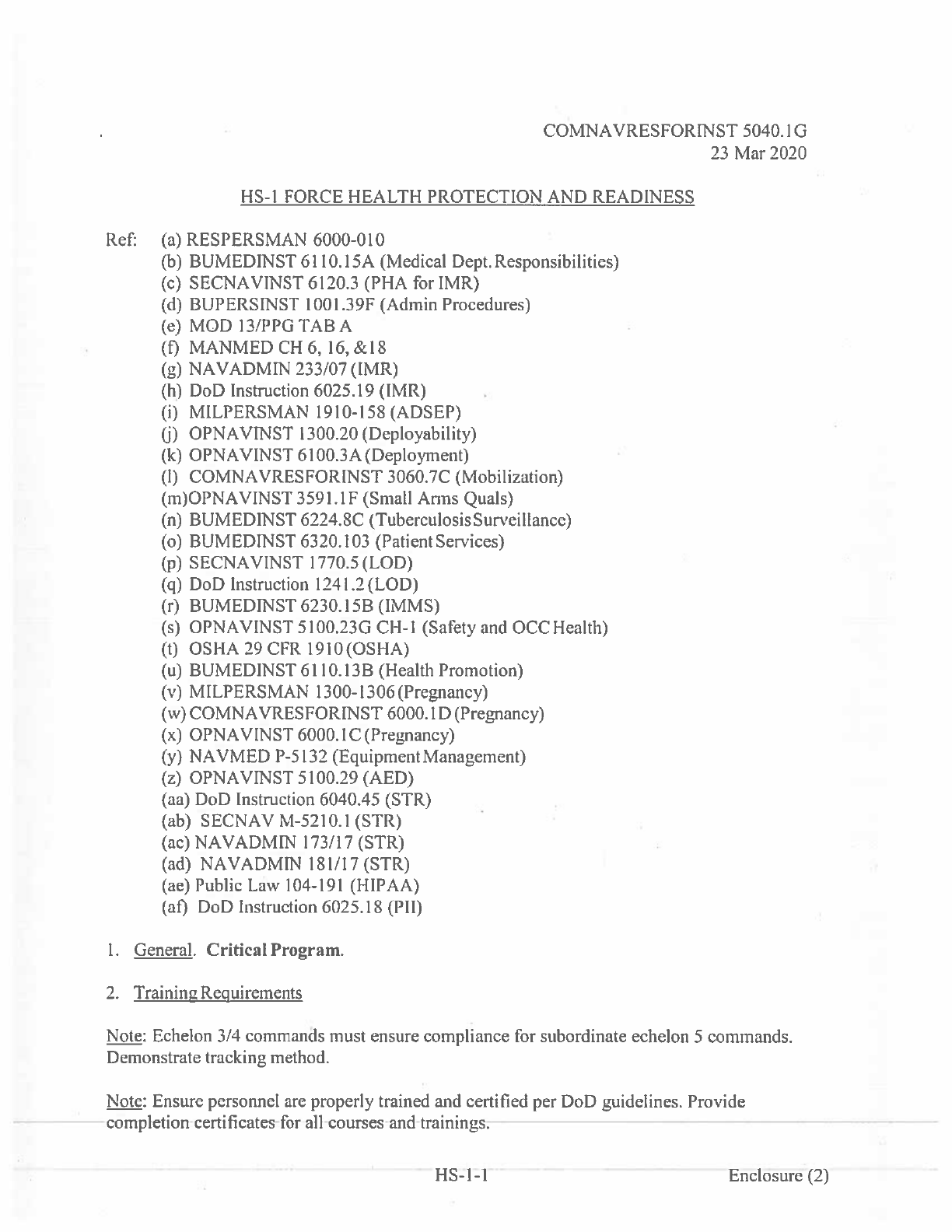
MS3
Temporarily Not Physically Qualified.
4
180 days
MILPERSMAN 6110-020 and RESPERSMAN 6000-010
MPC
Pregnant.
5
294 days
OPNAVINST 6000.1C
MPP
Non-deployable mother, child less than 12 months old or postpartum convalescence.
6
365 days #
OPNAVINST 6000.1C
MNN
Member who receives PRC-B per MILPERSMAN 6110-020 after submitting MRR package, will receive
the MNN MAS code, and requires a waiver for deployment greater than 30 days.
7
365 days
MILPERSMAN 6110-020 and RESPERSMAN 6000-010
MDT
Dental Class III which does not preclude mobilization.
8
180 days
SECNAVINST 6120.3 CH-1 and RESPERSMAN 6000-010
MDF
Dental Class IV which does not preclude mobilization.
9
180 days
SECNAVINST 6120.3 CH-1 and RESPERSMAN 6000-010
ADMIN
BCG
BUPERS Control Group. (BUPERS-83/911D use only.)
1
AKE
Key state/local employee. (COMNAVRESFORCOM use only.)
2
DoD Directive 1200.7 and BUPERSINST 1001.39F
AUP
Unsatisfactory participant. When administratively separating personnel, Enlisted members shall be
transferred to the Voluntary Training Unit, and Officers shall be transferred to the Active Status Pool.
3
180 days
RESPERSMAN 1001-010
ACR
Member has an approved conditional release from the Navy Reserves. Remove when conditional
release expires.
4
180 days
BUPERSINST 1001.39F and MILPERSMAN 1910-102
AAP
Administrative action pending which would preclude mobilization (e.g., unadjudicated ADMIN SEP
other than for UNSAT participation, NRA endorsing IRR request, etc.). Code applied upon
signature/submission to approval authority, and removed if request is denied.
5
180 days
RESPERSMAN 1001.5. If in question, contact RCC or
CNRFC N35.
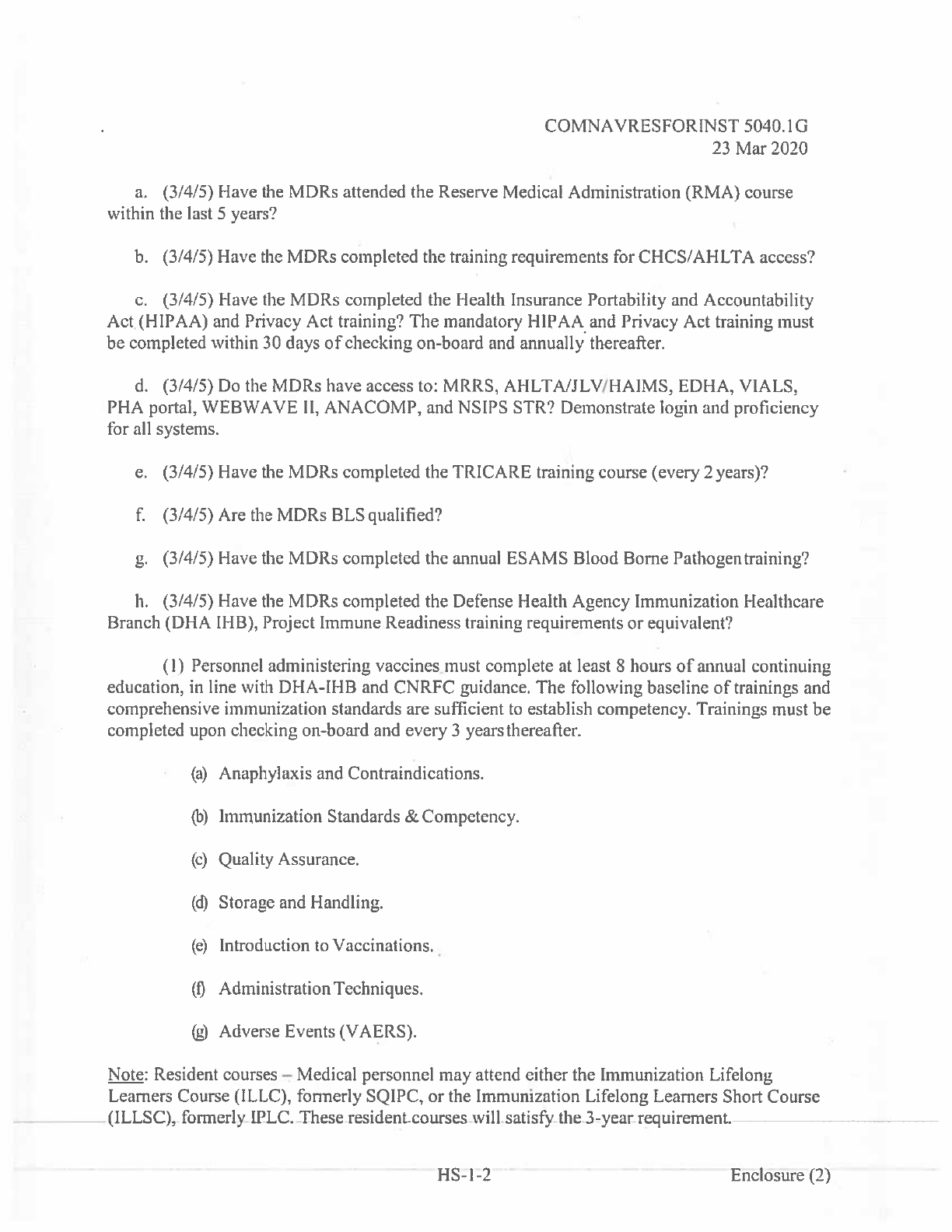
ASF
Member is ineligible for force protection duties.
6
Lautenberg Amendment, Section 922(g)(9) of Title 18,
U.S.C., DoDI 6400.06, and DD FORM 2760. See ASF def.
APB
Enlisted probationary drill status (UNSAT). NRA has six months to declare member in good drill
standing or ADSEP for UNSAT participation.
7
180 days
BUPERSINST 1001.39F, MILPERSMAN 1001-150, and
RESPERSMAN 1001-010
ARR
Retirement request submitted to NRA and pending approval from PERS-9, or retirement request
approved by PERS-9.
8
365 days
MILPERSMAN 1810-020
ACB
Not selected for continuation.
9
365 days
SECNAVINST 1920.7C and
http://www.public.navy.mil/bupers-
npc/career/reservepersonnelmgmt/officers/Pages/Con
tinuation.aspx
AS2
Member is within six months of HYT or statutory attrition.
10
180 days
Enlisted: MILPERSMAN 1160-120 and http://www
.public.navy.mil/bupers-npc/career/
reservepersonnelmgmt/enlisted/Pages/HYT.aspx.
Officer: SECNAVINST 1920.7C and
http://www.public.navy.mil/bupers-
npc/career/reservepersonnelmgmt/officers/Pages/Attr
itionRetirement.aspx
TS1
One-time 24 Month Deferment for affiliation. Member who affiliated within 0 to 183 days of release
from AC/FTS and is authorized a 24-month deferment from involuntary mobilization commencing on
the date of affiliation.
11
730 days #
NAVADMIN 145/19
AS1
One-time 12 Month Deferment for affiliation. Member who affiliated with prior military service and is
authorized a 12-month deferment from involuntary mobilization commencing on the date of
affiliation.
12
365 days #
NAVADMIN 145/19
ASO
Sole surviving son or daughter. May restrict mobilization locations.
13
DoDI 1315.18
AFP
Security Clearance issue. Joint Personnel Adjudication System (JPAS) records indicate derogatory
eligibility determination to include: Administrative Withdrawal, Loss of Jurisdiction, No Determination
Made, Revoked or Denied eligibility or currently reporting an active incident report.
14
365 days
DoD Directive 5200.2 and SECNAVINST M-5510.30
ASP
Member is a single parent or guardian, and requires a family care plan.
15
OPNAVINST 1740.4D and OPNAVINST 6000.1C
ASD
Member has an Active/Reserve military spouse and requires a family care plan.
16
OPNAVINST 1740.4D and OPNAVINST 6000.1C
AS3
Member is a non-custodial single parent who does not require a family care plan.
17
OPNAVINST 1740.4D and OPNAVINST 6000.1C
MPT
Member failed most recent PFA.
18
180 days
OPNAVINST 6110.1 (series), NAVADMIN 233/15, and
NAVADMIN 061/16
OAT
Members GTCC is suspended or revoked.
19
365 days
DoDI 5154.31, Vol 4
TRAINING
SAD
Approaching sanctuary. Member has 16 years or more of Active Duty. (COMNAVRESFORCOM use
only.)
1
OPNAVINST 1001.27
TMS
Attending authorized medical/dental/nursing school. Requires letter designating member has been
accepted into the program and BUMED RAO approval.
2
1460 days
RESPERSMAN 1570-020
DCO
Per OPNAVINST 1120.3B, Officers appointed under the direct appointment program will be required to
attend the Direct Commission Officer Indoctrination Course in Newport, Rhode Island, within 1 year of
appointment. Per RESPERSMAN 1200-010, DCO's shall use their first Annual Training (AT) to attending
DOIC. (COMNAVRESFORCOM use only.)
3
365 days
RESPERSMAN 1200-010/
COMNAVRESFORINST 1120.3
TBH
Member has not completed prescribed basic or reoccurring training to be considered qualified for
mobilization. Community managers shall manage the TBH MAS code and ensure the code is applied.
4
730 days
Each program is different. Need to review enlistment
documents or Navy Reserve Officer Service
Agreements. COMNAVCRUITCOMINST 1130.8 is a
starting point but community managers will have more
specific requirements. Also see RESPERMAN.
PRO
Officer authorized early release from AD to play sports. (COMNAVRESFORCOM use only.)
5
365 days
DoDI 1322.22
TS2
RP assigned to USMC unit, but has not received 2401 NEC
6
365 days
MCO 1730-6D
TRP
PRISE-R/designator or rate conversion training.
7
545 days
MILPERSMAN 1133-061
VS1
Member is on Definite (Temporary) Recall.
8
CNRFC
OWS
Member is on ADSW.
9
CNRFC
VOL
Member is a volunteer and fully available/ready for mobilization.
10
CNRFC
COMNAVRESFORINST
5040.IG
23
Mar2020
HS-1
FORCE
HEALTH
PROTECTION
AND
READINESS
Ref:
(a)
RESPERSMAN 6000-010
(b)
BUMEDINST
61
l0.15A
(Medical
Dept.
Responsibilities)
(c)
SECNAVINST
6120.3 (PHA for
IMR)
(d)
BUPERSINST
lOOl.39F
(Admin
Procedures)
(e)
MOD
13/PPGTABA
(F)
MANMED
CR
6,
16,&l8
(g)
NAVADMIN
233/07
(IMR)
(h)
DoD
Instruction
6025.19
(IMR)
(I)
MILPERSMAN
19
10-158
(ADSEP)
U)
OPNAVINST
1300.20
(Deployability)
(k)
OPNAVINST
61
00.3A
(Deploment)
(I)
COMNAVRESFORINST
3060.7C
(Mobilization)
(rn)OPNAVINST
3591.IF
(Small
Anns
Quals)
(n)
BUMEDINST
6224.8C
(Tuberculosis
Surveillance)
(o)
BUMEDINST
6320.103
(Patient
Services)
(p)
SECNAVINST
1770.5
(LOD)
(q)
DoD
Instruction
124
l.2(LOD)
(r)
BUMEDINST
6230.l5B
(IMMS)
(s)
OPNAVINST
5100.23G
CH-1
(Safety
and
0CC
Health)
(fl
OSHA
29
CFR
19l0(OSHA)
(u)
BUMEDINST
61
lO.13B
(Health
Promotion)
(v)
MILPERSMAN
1300-1306(Pregnancy)
(w)
COMNAVRESFORINST
6000.1
D
(Pregnancy)
(x)
OPNAVINST
6000.IC(Pregnancy)
(y)
NAVMED
P-S
132
(Equipment
Management)
(z)
OPNAVINST
5100.29
(AED)
(aa) DoD
Instruction
6040.45 (STR)
(ab)
SECNAV
M-52
10.1
(STR)
(ac)
NAVADMIN
173/17
(STR)
(ad)
NAVADMIN
181/17
(STR)
(ae)
Public
Law
104-191
(HIPAA)
(at)
DoD
Instruction 6025.18
(P11)
I.
General.
Critical Program.
2.
Training
Requirements
Note: Echelon
3/4
commands
must
ensure
compliance
for
subordinate
echelon
5
commands.
Demonstrate
tracking
method.
Note:
Ensure
personnel
are
properly
trained
and
certified
per
DoD
guidelines.
Provide
completion
certificates
for
all
courses
and
trainings.
HS-l-1
Enclosure
(2)
COMNAVRESFORINST
5040.1G
23
Mar 2020
a.
(3/4/5) Have
the
MDRs
attended
the
Reserve
Medical
Administration
(RMA)
course
within
the last
5
years?
b.
(3/4/5)
Have
the
MDRs
completed
the
training
requirements
for
CHCS/AHLTA
access?
c.
(3/4/5)
Have
the
MDRs
completed
the Health
Insurance
Portability
and
Accountability
Act.
(HIPAA)
and
Privacy
Act
training? The
mandatory
HIPAA
and
Privacy
Act
training
must
be
completed
within
30
days
of
checking
on-board
and
annually
thereafter.
d.
(3/4/5)
Do
the
MDRs have
access
to:
MRRS,
AHLTA/JLV/HAIMS,
EDNA,
VIALS,
PHA
portal,
WEBWAVE
II,
ANACOMP,
and
NSIPS
STR?
Demonstrate
login
and
proficiency
for
all
systems.
e.
f.
g.
It
Branch
(3/4/5)
Have
the
MDRs
completed
the
TRICARE
training
course
(every
2
years)?
(3/4/5)
Are
the
MDRs
BLS
qualified?
(3/4/5)
Have
the
MDRs
completed
the
annual
ESAMS
Blood
Borne
Pathogentraining?
(3/4/5)
Have
the
MDRs
completed
the
Defense Health
Agency Immunization
Healthcare
(DHA
IHB),
Project
Immune
Readiness
training
requirements
or
equivalent?
(I)
Personnel
administering
vaccines
must
complete
at
least
8
hours
of
annual
continuing
education,
in
line
with
DHA-IHB
and
CNRFC guidance.
The
following
baseline
of
trainings
and
comprehensive immunization
standards
are
sufficient
to
establish
competency.
Trainings
must
be
completed
upon
checking
on-board
and
every
3
years
thereafter.
(a)
Anaphylaxis
and
Contraindications.
Immunization
Standards
&
Competency.
Quality
Assurance.
Storage
and
Handling.
(e)
Introduction
to
Vaccinations.
(1)
Administration
Techniques.
(g)
Adverse
Events
(VAERS).
Note:
Resident
courses
-
Medical
personnel
may
attend
either
the
Immunization
Lifelong
Learners
Course
(ILLC),
formerly
SQIPC,
or
the
Immunization
Lifelong Learners
Short
Course
(ILLSC),
formerly
IPLC.
These
resident
courses
will
satis&
the
3-year
requirement.
HS-1-2
Enclosure
(2)
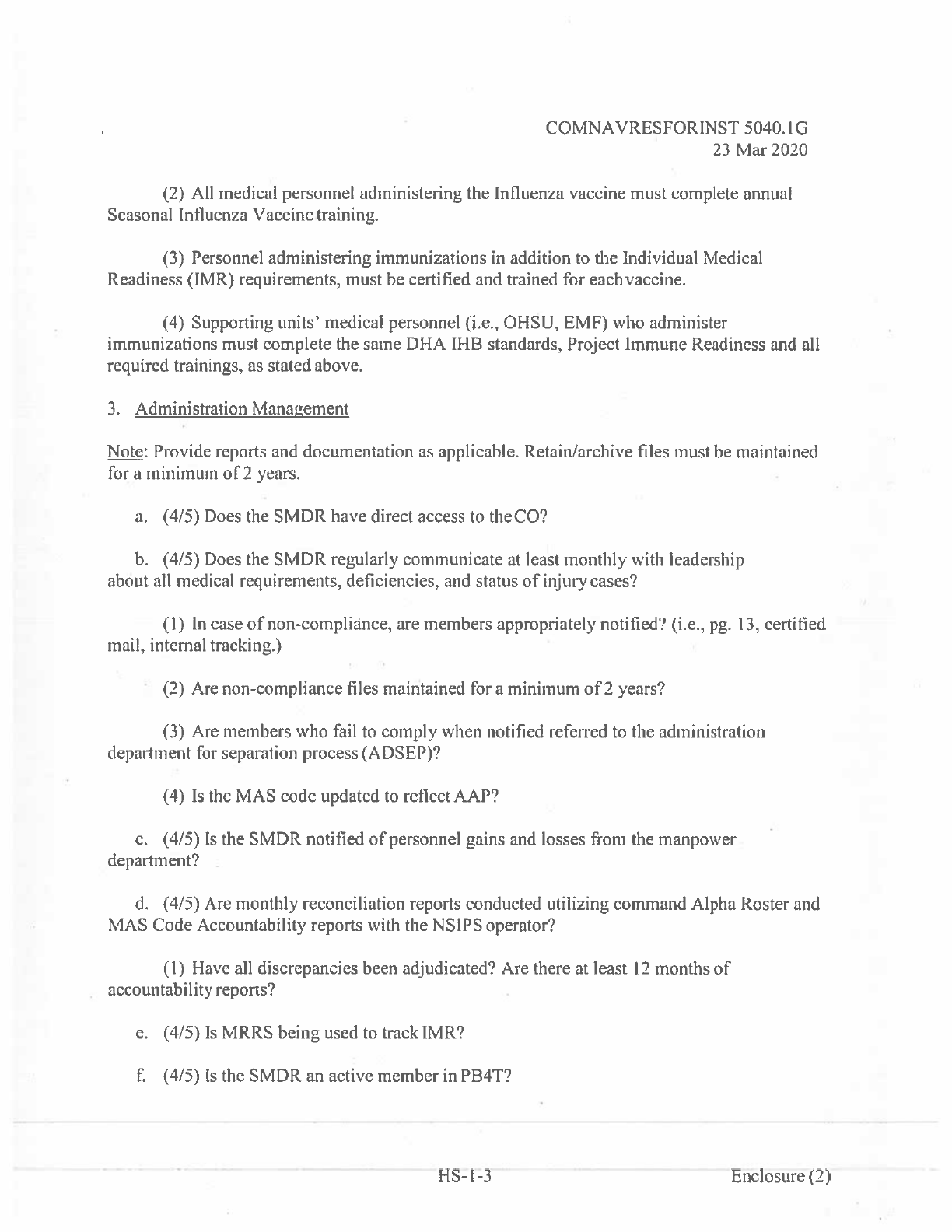
COMNAVRESFORINST
5040.IG
23
Mar2020
(2)
All
medical
personnel
administering
the
Influenza
vaccine
must
complete
annual
Seasonal
Influenza
Vaccine
training.
(3)
Personnel
administering immunizations
in
addition
to
the
Individual
Medical
Readiness (IMR)
requirements, must
be
certified
and
trained
for
eachvaccine.
(4)
Supporting
units’
medical
personnel
(i.e.,
OHSU,
EME)
who
administer
immunizations
must
complete
the
same
DNA
IHB
standards, Project
Immune Readiness
and
all
required trainings,
as
stated
above.
3.
Administration
Management
Note:
Provide reports
and
documentation
as
applicable.
Retain/archive
files must
be
maintained
for
a
minimum
of
2
years.
a.
(4/5)
Does
the
SMDR
have
direct
access
to
the CU?
b.
(4/5)
Does the
SMDR
regularly communicate
at
least
monthly
with
leadership
about
all
medical
requirements,
deficiencies,
and
status
of
injury cases?
(I)
In
case
of
non-compliance,
are
members
appropriately
notified?
(i.e.,
pg.
13,
certified
mail,
internal
tracking.)
(2)
Are
non-compliance
files
maintained
for
a
minimum
of
2
years?
(3)
Are
members
who
fail
to
comply
when
notified referred
to
the
administration
department
for
separation process
(ADSEP)?
(4)
Is
the
MAS
code
updated
to
reflect
AAP?
c.
(4/5)
Is
the
SMDR
notified
of
personnel
gains
and
losses
from
the
manpower
-
department?
d.
(4/5)
Are
monthly
reconciliation
reports
conducted
utilizing
command Alpha
Roster
and
MAS
Code
Accountability
reports
with
the
NSIPS
operator?
(1)
Have
all
discrepancies
been
adjudicated?
Are
there
at
least
12
months
of
accountability
reports?
e.
(4/5)
Is
MRRS
being
used
to
track
IMR?
f.
(4/5)
Is
the
SMDR
an
active
member
in
PB4T?
HS-l-3
Enclosure
(2)
COMNAVRESFORINST
5040.IG
23
Mar
2020
g.
(4/5)
Is
there
a
current
self-assessment
on
file
(12
months) utilizing
the
most
current
assessment
guide?
It
(4/5)
Does the
SMDR have
a
current
assumption
of
duty
letter,
and
an
all-inclusive
medical
department
turnover
assessment
on
file?
(1)
The
turnover
assessment
should
include
a
comprehensive
evaluation
of
the status
of
the medical
department
within
30
days
of
assumption
ofduty.
I.
(4/5)
Is
there
documentation
of
all
physical
examinations
completed?
j.
(4/5)
Is
there
a
medical
department
Standard
Operating
Procedures
(SOP) binder?
SOP
should
include
a
minimum
of:
Note:
Regions
and
activities
may
develop
their
own
SOPs.
The SOPs
should
incorporate
local
DoD MTFs’
guidance, processes,
and
protocols
as
applicable
for
some
required
sections.
(I)
Supporting
OHSU/EMF
unit
POCs,
local
Military
Treatment
Facilities
(MTF),
etc.
(2)
Procedures
for
contacting
Emergency
Medical
Sen’ices(EMS).
(3)
Accidental needle
stick
protocol.
(4)
Biohazard
collection,
transfers,
spill
procedures,
and
infection
control.
(5)
Immunization
cold
chain
management
(normal
routine/duty
routine).
(6)
Anaphylaxis
response
plan.
(7)
Procedures
for
Vaccine Adverse
Event
Reporting
Systern(VAERS).
(8)
Procedures
for
conducting/processing
blood
work.
(9)
Defense Health
Agency
Great
Lakes
(DHA-GL) processes
and
procedures.
Note:
Maintain
DHA-GL worksheets
for
36
months.
4.
Individual
Medical
Readiness(IMR)
Note:
Provide
MRRS
reports
and
documentation
as
applicable.
a.
(4/5)
Does
the
IMR
meet
or
exceed
the
followingcriteda?
(1)
FullyMedicallyReady
85%.
HS-1-4
Endosure
(2)
COMI’1AVRESFORINST
5040.IG
23
Mar2020
(2)
Partially
Medically
Ready
:S
5%.
(3)
Medically
Ready
Indeterminate
:55%.
(4)
Not
Medically
Ready
:5
5%.
(5)
Full
+
Partial
Medical
Readiness
0
90%.
b.
(4/5)
Does
dental
readiness
reflect
current
standards?
(reference(g))
(I)
Number
of
Dental
Class
I
=
(2)
Number
of
Dental
Class
II
=_______
(3)
Number
of
Dental
Class
III
=
(4)
Number
of
Dental
Class
IV
=________
5.
Service
Treatment
Records
(STR1
Management
—-
Note:
Provide
MRRS
reports
and
documentation
as
applicable.
Retain/archive
files
must
be
maintained
for
a
minimum
of
2
years.
a.
(4/5)
Where
are the
STRs
maintained,
and
is
security
ofSTRs
preserved?
b.
(4/5)
Are
STRs
(medical/dental)
properly
tiled?
c.
(4/5)
Is
there
a
STR
for
each
member,
and
are
they
in
current
jackets
and
good
condition?
d.
(4/5)
Is
STRs’
inventory
conducted
quarterlyand
retained
on
file?
e.
(4/5) Are
NAVMED
6
150/7
(Pink Cards)
used
as
STR
placeholder
foraccountability?
f.
(4/5)
Does
MRRS
and
AHLTA data
reflect
the
same
information
in
the STRs?
g.
(4/5)
Are
STRs
verified
annually
(MRRS
and
AHLTA
data),
and
more
ofienas
applicable’?
(check-in,
check-outs,
MOBs,
and
PHAs)
h.
(4/5)
Are
laboratory
results
filed
in
section
IV
for
G6PD,
sickle
cell,
and
blood
type?
i.
(4/5) Are
physical
examinations
and
PHAs
reviewed
for
completeness
and
accuracy?
HS-I-5
Enclosure
(2)
COMNAVRESFORINST
5040.1
G
23
Mar2020
j.
(4/5)
Have
medical
warning
tags
been
documented
in
MRRS,
issued
to
personnel
who
require
them
and filed
accordingly?
k.
(4/5) Are
STRs
retired/transferred
per
current guidance?
(NSIPS
STR
tracking database)
1.
(4/5) Are
transmittal
forms
DD
2963
submitted within
5
days
of
members’
separating?
m.
(4/5) Are
DD
2963
attached
to
STRs
when
transferred
to
Navy
MedicineRecords
Activity
(NMRA)
and
ANACOMP?
n.
(4/5) Are
NSIPS
loss
reports
submitted
to
the
echelon
4
N9
department
with
amplifying
information
on the
status
of
the
separating
STRs?
o.
(4/5)
Is
CNRFC’s
N9
STR
tracker
updated
weekly
as
per
current
guidance?
6.
Health
Protection/Immunizations
Note:
Provide
documentation
and
reports
as
applicable.
Retain/archive
files
must
be
maintained
for
a
minimum
of
2
years.
a.
(4/5)
Anaphylaxis
Management
(1)
In
the
event
of
an
adverse immunization
reaction,
is
there
a
pocket
mask
and
EPI
PEN
on
station?
(2)
Can
the
MDRs
demonstrate
proficiency
to
treat
anaphylaxis?
b.
(4/5)
Immunization
Management
(I)
Does
the
medical
department
have
an
appropriate
BIOMED
refrigerator
for
the
storage
of
vaccines?
(2)
Is
the
refrigerator
identified
as
“Biological/Immunization
Storage
Only,
No
Food
or
Drinks”
and
actually
void
of
food and
drinks?
(3)
Is
refrigerator
monitored
for
temperature
control?
(a)
Is
a
Sensaphone
in
place
and
alarm tested
at
least
monthly?
Are
batteries replaced
as
per
manufactures’ specifications?
)
Does
Sensaphone
have
a
stand-alone
phone
line?
(c)
Does
the
MDRs
and
duty personnel
monitor
and
record
refrigerator temperatures?
HS-l-6
Enclosure
(2)

COMNAVRESFORINST
5040.1
G
23
Mar2020
(4)
Are
the
MDRs
monitoring immunization
expiration
dates?
(5)
Are
Vaccine
Information Sheets
(VIS)
available
andcurrent?
(6)
Are
MRRS
deferred
immunizations
valid and
properly
diagnosed
by
a
credentialed
health
care
provider?
7.
PHA/MHA
Management
Note:
Provide
documentation
and
reports
as
applicable.
Retain/archive
files
must be
maintained
for
a
minimum
of
2
years.
a.
(4/5)
Is
leadership
notified
in
advance
(preferably
90
days)
of
personnel due
for
a
PHA
and
annual
Mental
Health
Assessments
(MHA)?
Explain
notification
process.
b.
(4/5)
Are
members completing
annual
MHAs
and
receiving
appropriatereferrals?
8.
Deployment
Health
Management
a.
(4/5)
Assess
the
state
of
health
after
deployment outside
the
United
States
in
support
of
military operations
and
identify
present
and
future medical
care.
Note:
Provide
documentation
and
reports
as
applicable.
Retain/archive
files
must
be
maintained
for
a
minimum
of
2
years.
(I)
Are
members
completing
the
required
Pre-DHA
DD
2795,
Post-DHA
DD
2796,
and
PDHRA
DD
2900
when due?
(a)
Current
month
PDHRA
status:_________________
(b)
Total
Due:_________________
(c)
Compliant:
•
Completed
(not
certified):
(2)
Enter
PDHRA
combined
totals
for
the past
3
months
below:
(a)
PDHRAs
>
30d___________
)
PDHRAs
30-15d__________
(c)
PDHRAs
<
15d
HS-l-7
EPtlosUIe(2)
COMNAVRESFORINST
5040.1
G
23
Mar
2020
PDHRAs
overdue__________
(3)
Are
all
required
deployment
health
assessment screenings
completed
via
EDHA,
documented
in
MRRS,
and
placed
in
members’
STRs?
(4)
Are
members
found
not
fit
on
the
Pre-DHA
placed
in
an
appropriate injury
case
management
status?
(5)
Are
Post-DRA
and
Post-DHRA
referrals
managed
properly
through
LOD
process?
(6)
Is
the Plan
of
the
Month (POM)
or
other
correspondence
used
to
spotlight
deployment
health
resources
such
as
Psychological
Health
Outreach
Program (PHOP)
or
Return
Warrior
Workshops
(RWW),
on-site
activities,
and
call
center
events?
9.
Medical
Mobilization
Screening
Note:
Provide
documentation
and
reports
as
applicable.
Retain
files
must
be
maintained
for
a
minimum
of
2
years.
a.
(4/5)
Is
NAVMED
1300/4
initiated
upon
members’
notification
(RCI
date)
of
mobilization?
b.
(4/5)
Is
NAVMED
1300/4
completed
within
60
days
of
deployment
notification
(RC2
date)?
c.
(4/5)
Are
AOR
medical
waivers submitted
to
appropriate
AOR
surgeon
via
the
RCC?
d.
(4/5)
Are
small
arms
waivers completed
and
approved prior
to
members’
departure
for
ECRC?
10.
Injury
Case
Management
:
Provide
documentation
and
reports.
Injury cases
retain
files
must
be
maintained
for
a
minimum
of
2
years.
a.
(4/5)
Medical
Retention
Review
(MRR)
Management
(1)
#
of
MRR
NPQ/RR
cases:_______
(2)
#
of
overdue
MRR
NPQ/RR
cases:_______
(3)
Are
MRR
cases
effectively managed
and
updated
in
MRRS
to
reflect
current
status?
(4)
Is
a
signed
pg.
13
and
a
MRRS generated
SF 600
available
for
each
MRR
case
file?
HS-l-8
Enclosure
(2)
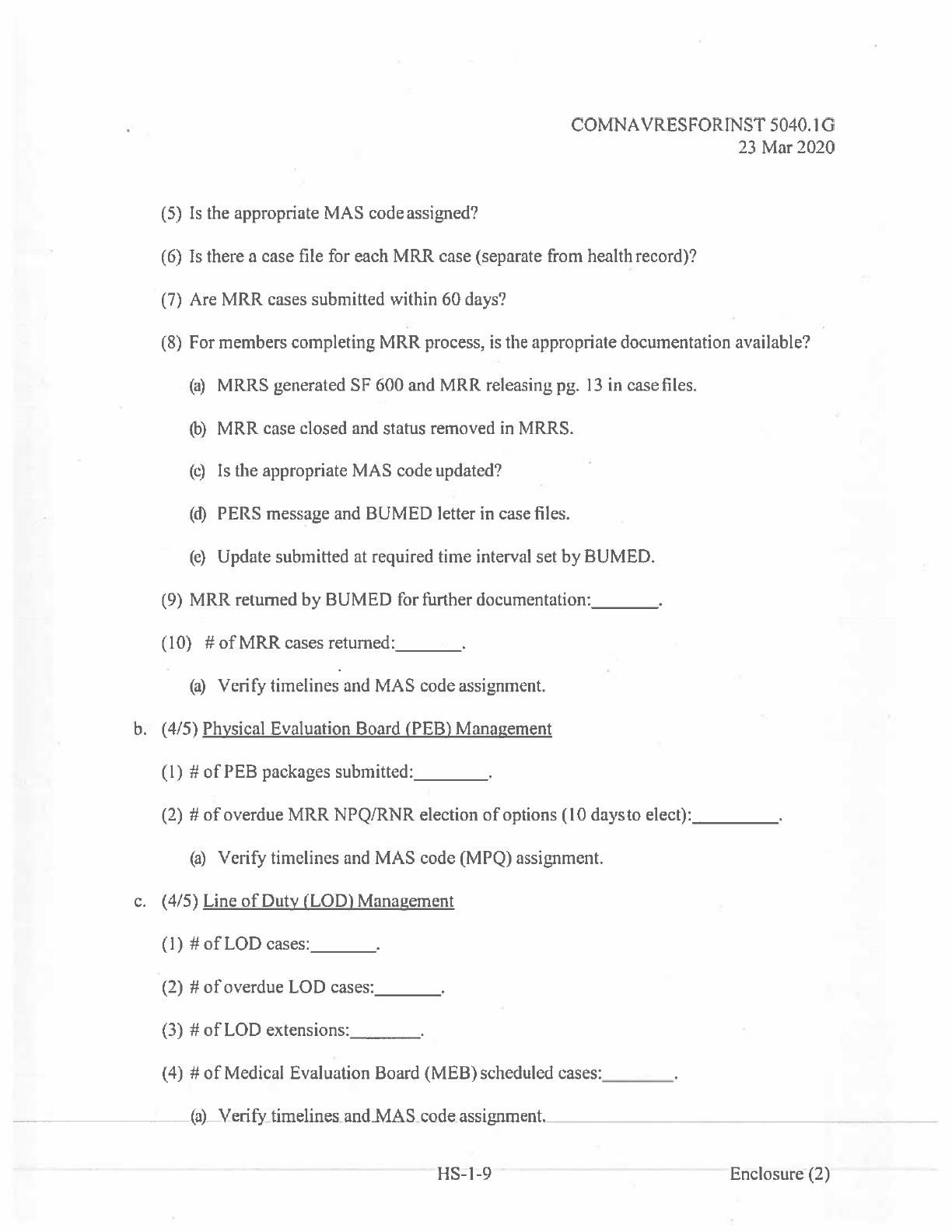
COMNAVRESFORINST
5040.IG
23
Mar 2020
(5)
Is
the
appropriate
MAS
code assigned?
(6)
Is
there
a
case
file for
each
MRR
case
(separate
from
health
record)?
(7)
Are
MRR
cases
submitted
within
60
days?
(8)
For
members
completing
MRR process,
is
the
appropriate documentation available?
(a)
MRRS
generated
SF
600
and
MRR
releasing
pg.
13
in
case
files.
0’)
MRR
case
closed
and
status
removed
in
MRRS.
(c)
Is
the
appropriate
MAS
code
updated?
(M
PERS
message
and
BUMED letter
in
case
files.
(e)
Update
submitted
at
required
time
interval
set
by BUMED.
(9)
MRR
returned
by BUMED
for
further
documentation:_______
(10)
#
of
MRR
cases
returned:_______
(a)
Verify
timelines
and
MAS
code
assignment.
b.
(4/5)
Physical
Evaluation
Board
(PEB)
Management
(I)
#
of
PEB
packages
submitted:________
(2)
#
of
overdue
MRR
NPQ/RNR
election
of
options
(10
daysto
elect):__________
(a)
Verify
timelines
and
MAS
code (MPQ)
assignment.
c.
(4/5)
Line
of
Duty (LOD)
Management
(1)
#ofLOD
cases:______
(2)
#
of
overdue
LOD
cases:________
(3)
#
of
LOD
extensions:________
(4)
#
of
Medical
Evaluation
Board
(MEB)
scheduled
cases:________
(a)
Verify
timelines
and
MAS
code assignment.
1-15-1-9
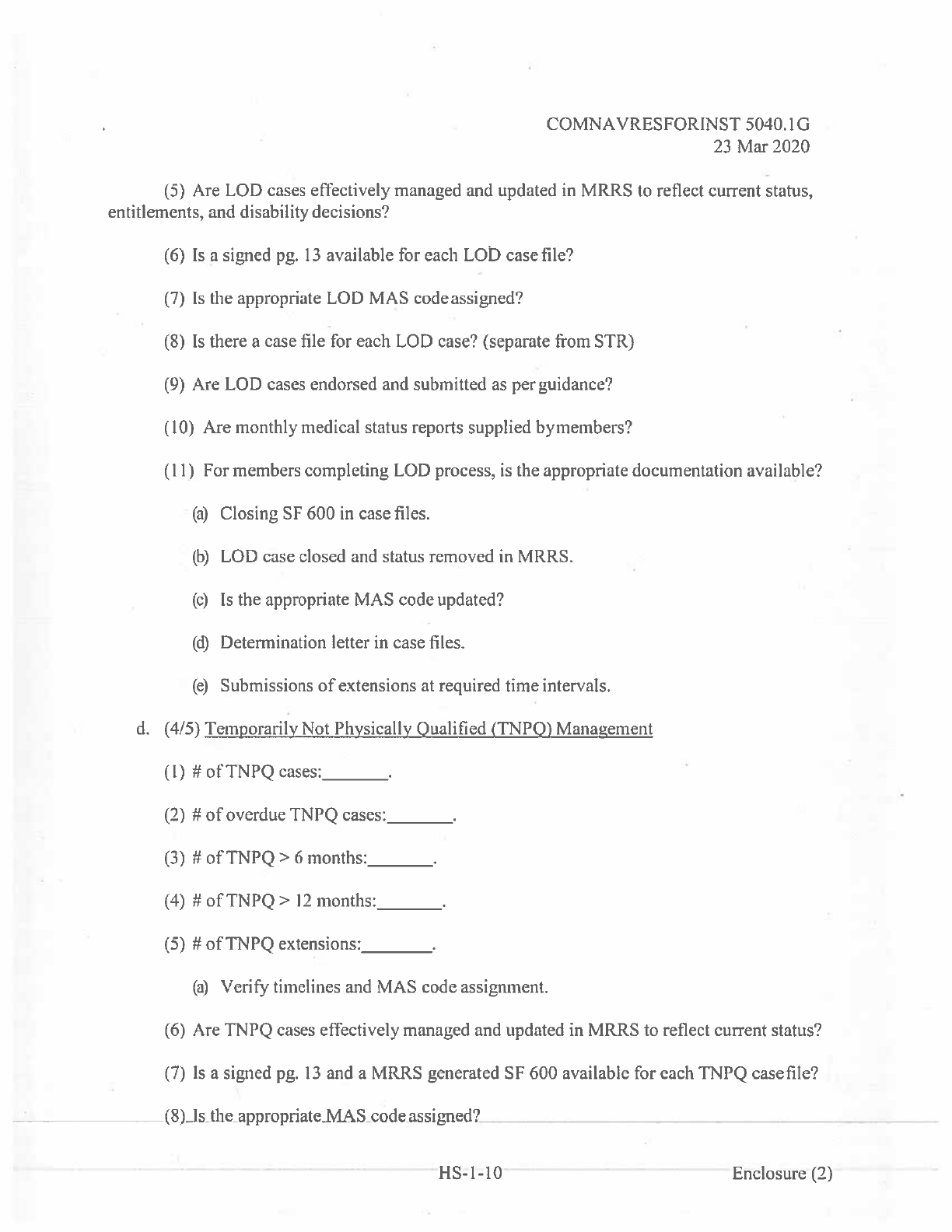
COMNAVRESFORINST
5040.1
G
23
Mar2020
(5)
Are
LOD
cases
effectively
managed
and
updated
in
MRRS
to
reflect
current
status,
entitlements,
and
disability decisions?
(6)
Is
a
signed
pg.
13
available
for
each
LOD
case
file?
(7)
Is
the
appropriate
LOD MAS
code
assigned?
(8)
Is
there
a
case
file
for
each
LOD
case?
(separate
from STR)
(9)
Are
LOD
cases
endorsed
and
submitted
as
per guidance?
(10)
Are
monthly
medical
status reports supplied
bymembers?
(II)
For
members
completing
LOD
process,
is
the
appropriate documentation
available?
(a)
Closing
SF
600
in
case
files.
(b)
LOD
case
closed
and
status removed
in
MRRS.
(c)
Is
the
appropriate
MAS
code updated?
(d)
Determination letter
in
case
files.
(e)
Submissions
of
extensions
at
required
time
intervals.
d.
(4/5)
Temporarily
Not
Physically
Qualified
(TNPQ)
Management
(l)#otTNPQtases
______
(2)
#
of
overdue
TNPQ
cases
_______
(3)
#
of
TNPQ
>6
months:______
(4)
#
of
TNPQ>
12
months:______
(5)
#
of
TNPQ
extensions
________
(a)
Verify
timelines
and
MAS
code
assignment.
(6)
Are
TNPQ
cases
effectively
managed
and
updated
in
MRRS
to
reflect
current
status?
(7)
Is
a
signed
pg.
13
and
a
MRRS
generated
SF
600
available
for
each
TNPQ
caseflle?
(8)
Is
the
appropriate
MAS
code
assigned?
HS-
1-10
Enclosure
(2)

COMNAVRESFORINST
5040.!
G
23
Mar 2020
(9)
Is
there
a
case
file
for
each
TNPQ
case
(separate
from
health
record)?
(!0)
Are
monthly
updates
supplied
by
members?
(!l)
Are
TNPQ>
6
months
monitored
and
submitted
for
extension,
conversion
to
MRR
or
ADSEP
process?
(!2)
Are
TNPQ
>
!
2
months
monitored
and
submitted
for
conversion
to
MRR
or
ADSEP
process?
(!3)
For
members
completing
TNPQ
process,
is
the
appropriate
documentation
available?
(a)
SF
600
and
TNPQ
releasing
pg.
!3
in
casefiles.
(b)
TNPQ
case
closed
and
status
removed
in
MRRS.
(c)
Is
the
appropriate
MAS
code
updated?
e.
(4/5)
Temporarily
Not
Dentally
Qualified
(TN
DO)
Management
(1)
#
ofTNDQ
cases:_______
(2)
#
of
overdue
TNDQ
cases:________
(3)
#
of
TNDQ
>6
months:_______
(4)
#ofTNDQ>
12
months:______
(5)
#
ofTNDQ
extensions:________
(a)
Verify
timelines
and
MAS
code
assignment.
(6)
Arc
TNDQ
cases
effective!y
managed
and
updated
in
MRRS
to
reflect
current
status?
(7)
Is
a
signed
pg.
13
and
a
MRRS
generated
SF
600
available
for
each
TNDQ
case
file?
(8)
Is
the
appropriate
MAS
code
assigned?
(9)
Is
there
a
case
file
for each
TNDQ
case
(separate
from
health
record)?
(10)
Are
monthly
updates
supplied
bymembers?
HS-1-1
I
Enclosure(2)
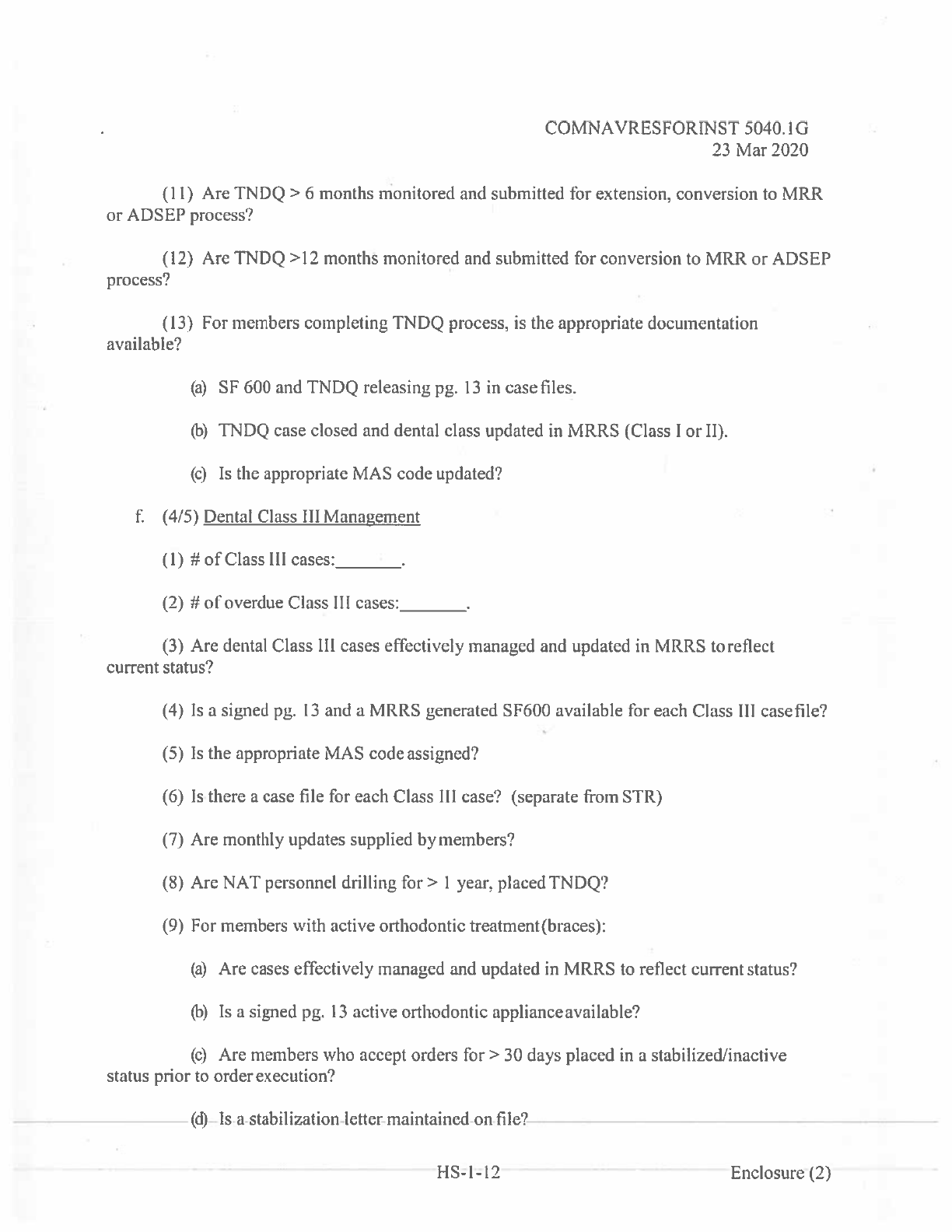
COMNAVRESFOR[NST
5040.1
G
23
Mar2020
(II)
Are
TNDQ>
6
months
monitored
and
submitted
for
extension,
conversion
to
MRR
or
ADSEP process?
(12)
Are
TNDQ
>12
months
monitored
and
submitted
for
conversion
to
MRR
or
ADSEP
process?
(13)
For
members
completing
TNDQ
process,
is
the
appropriate
documentation
available?
(a)
SF
600 and
TNDQ
releasing
pg.
13
in
case
files.
(b)
TNDQ
case
closed
and
dental
class
updated
in
MRRS
(Class
I
or
II).
(c)
Is
the
appropriate
MAS
code
updated?
t:
(4/5)
Dental
Class
III
Management
(I)
#ofClass
Ill
cases:_______
(2)
#
of
overdue
Class
Ill
cases:________
(3)
Are
dental
Class
Ill
cases
effectively
managed
and
updated
in
MRRS
toreflect
current
status?
(4)
(5)
(6)
(7)
(8)
(9)
Is
a
signed
pg.
13
and
a
MRRS
generated
SF600
available
for
each
Class
Ill
casefile?
Is
the
appropriate
MAS
code
assigned?
Is
there
a
case
file for
each
Class
Ill
case?
(separate
from
STR)
Are
monthly updates
supplied
by
members?
Are
NAT
personnel
drilling
for>
I
year,
placed
TNDQ?
For
members
with
active
orthodontic
treatment
(braces):
(a)
Are
cases
effectively managed
and
updated
in
MRRS
to
reflect
current
status?
(b)
isa
signed
pg.
13
active
orthodontic
applianceavailable?
(c)
Are
members
who
accept
orders
for>
30
days
placed
in
a
stabilized1inactive
status
prior
to
order
execution?
(d)
Is
a
stabilization
letter
maintained
on
file?
HS-l-12
Enelosure{2)
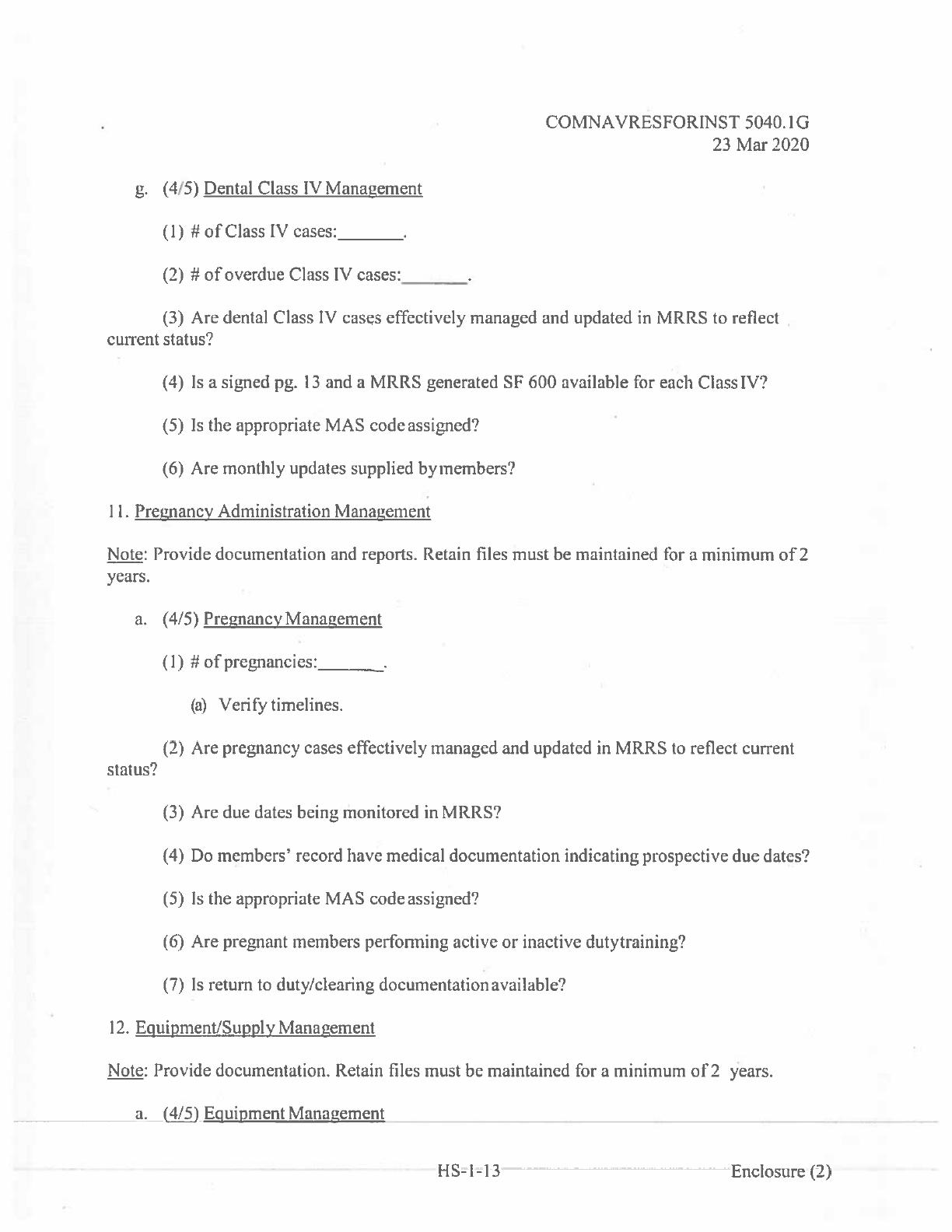
COMNAVRESFORINST
5040.!
G
23
Mar
2020
g.
(4/5)
Dental
Class
IV
Management
(I)
#of
Class
IV
cases:_______
(2)
#
of
overdue
Class
IV
cases:________
(3)
Are
dental
Class
IV
cases
effectively
managed
and
updated
in
MRRS
to
reflect
current
status?
(4)
Is
a
signed
pg.
13
and
a
MRRS
generated
SF
600
available
for
each
Class
IV?
(5)
Is
the
appropriate
MAS
code
assigned?
(6)
Are
monthly
updates
supplied
byrnembers?
II.
Pregnancy
Administration
Management
Note:
Provide
documentation
and
reports.
Retain
files
must
be
maintained
for
a
minimum
of
2
years.
a.
(4/5)
Pregnancy
Management
(1)
#ofpregnancies:
—.
(a)
Verify timelines.
(2)
Are
pregnancy
cases
effectively
managed
and
updated
in
MRRS
to
reflect
current
status?
(3)
Are
due
dates
being
monitored
in
MRRS?
(4)
Do
members’
record
have
medical
documentation
indicating
prospective
due
dates?
(5)
Is
the
appropriate
MAS
code
assigned?
(6)
Are
pregnant
members
performing
active
or
inactive
dutytraining?
(7)
Is
return
to
duty/clearing
documentationavailable?
12.
Equipment/Supply
Management
Note:
Provide
documentation.
Retain
files
must be
maintained
for
a
minimum
of
2
years.
a.
(4/5)
Equipment Management
HS-l-13
Enclosure
(2)
COMNAVRESFORINST
5040.IG
23
Mar
2020
(I)
Is
medical
diagnostic
equipment managed
and
maintained
as
perrnanufacwrer’s
specifications?
(2)
Are
applicable
BIOMED
certifications,
calibration,
and
repairs
documented
and
maintained?
Expiration
dates
monitored?
(3)
Is
there
an
AED
available
on
each
floor?
Are
AEDs
beingtested?
(4)
Is
there
a
Chinook
medical
kit
available
on
each
floor?
Expiration dates
monitored?
b.
(4/5)
Supply
Manauement
(1)
Are
medical
consumables
inventoried
and
managed
with
the
supply
department?
(2)
Is
the
budget
adequate
to
accomplish
the
mission?
13.
Health
Promotion
and
Wellness
Protzram.
To
establish policy
and
assign
responsibilities
for
the Navy
and
Marine Corps
Health
Promotion
and
Wellness
(HPW)
Program.
in
supports
the
CNO’s
“Sailor
2025”
initiative.
Note:
Provide
documentation.
a.
(4/5)
Health
Promotion
Management
(I)
Is
a
Command
Health
Promotion
Coordinator
(HPC)
appointed/designated
in
writing
to
serve
as
the
principal
advisor
for
health
promotion
services?
(2)
As
the
HPC
completed
(within
60
days
of
appointment)
the
Navy
Health
Promotion
Basics
course
online
or
attended
other
Navy
health
promotion
courses?
(3)
Are
HPC
assistants
identified/designated
in
writing?
(4)
Is
a
health
promotion
committee
established?
(5)
Are
monthly
health
promotions
activities
and
observances implemented?
(6)
Are
health
promotions
literacy
resources
readily
available
and
displayed
in
common
areas?
(i.e.,
pamphlets,
catalogs, brochures,
posters).
(7)
Is
the
POM
or
other
routine
correspondence
used
to
spotlight
health
promotion
activities,
health
fairs
and
local
events?
(8)
Is
the
Blue-H
Navy
Surgeon
General’s
Health
Promotion
and
Wellness
Award
being
submitted?
l-IS-l-14
Enclosure
(2)
